

Enhanced recovery after surgery (ERAS) or fast-track pathways are well established across a wide range of surgical procedures and demonstrate consistent success in decreasing surgical stress, maintaining physiological homeostasis and expediting postoperative recovery (Ljungqvist et al, 2017)(Box 1).
Box 1.Clinical resources
- National Institute for Health and Care Excellence. Perioperative care in adults. Evidence review for enhanced recovery programmes. 2020. https://tinyurl.com/3z3hvh79
- American Association of Nurse Anesthesiology. 2022. Enhanced recovery after surgery. 2022. https://tinyurl.com/mm562fsk
- ERAS Society. Enhanced recovery after surgery. 2022. https://erassociety.org
The implementation of ERAS has reduced hospital lengths of stay and surgical complications, so the focus is now on accelerating post-discharge functional recovery and rehabilitation (Kehlet, 2020). Incomplete postoperative recovery, with residual cognitive impairment, sarcopenia and chronic pain for example, will limit the restoration of health and may increase the risk of long-term morbidity (Kehlet, 2020; Myles, 2020).
To help the implementation of ERAS pathways, the ERAS Society (2022) guidelines, which integrate evidence-based practices into multimodal care pathways, have been published for multiple surgical specialties, leading each profession within the surgical team, including nursing, to reconsider their roles and best practice. However, areas of postoperative recovery on the ward and post-discharge rehabilitation are still to be clearly defined in many clinical guidelines.
The success of ERAS is reliant upon fulfilment of the clinical protocol and buy-in from all professions involved in the surgical journey. However, in studies evaluating adherence to ERAS components, poor compliance to protocols is observed mostly in areas of care that are delivered once patients have returned to the ward (Roulin et al, 2017; Aarts et al, 2018). For example, despite the widely recognised importance of early mobilisation as part of ERAS programmes, compliance with mobilisation goals has been reported to be suboptimal in studies of systematic ERAS implementation (Maessen et al, 2007; Kehlet, 2018).
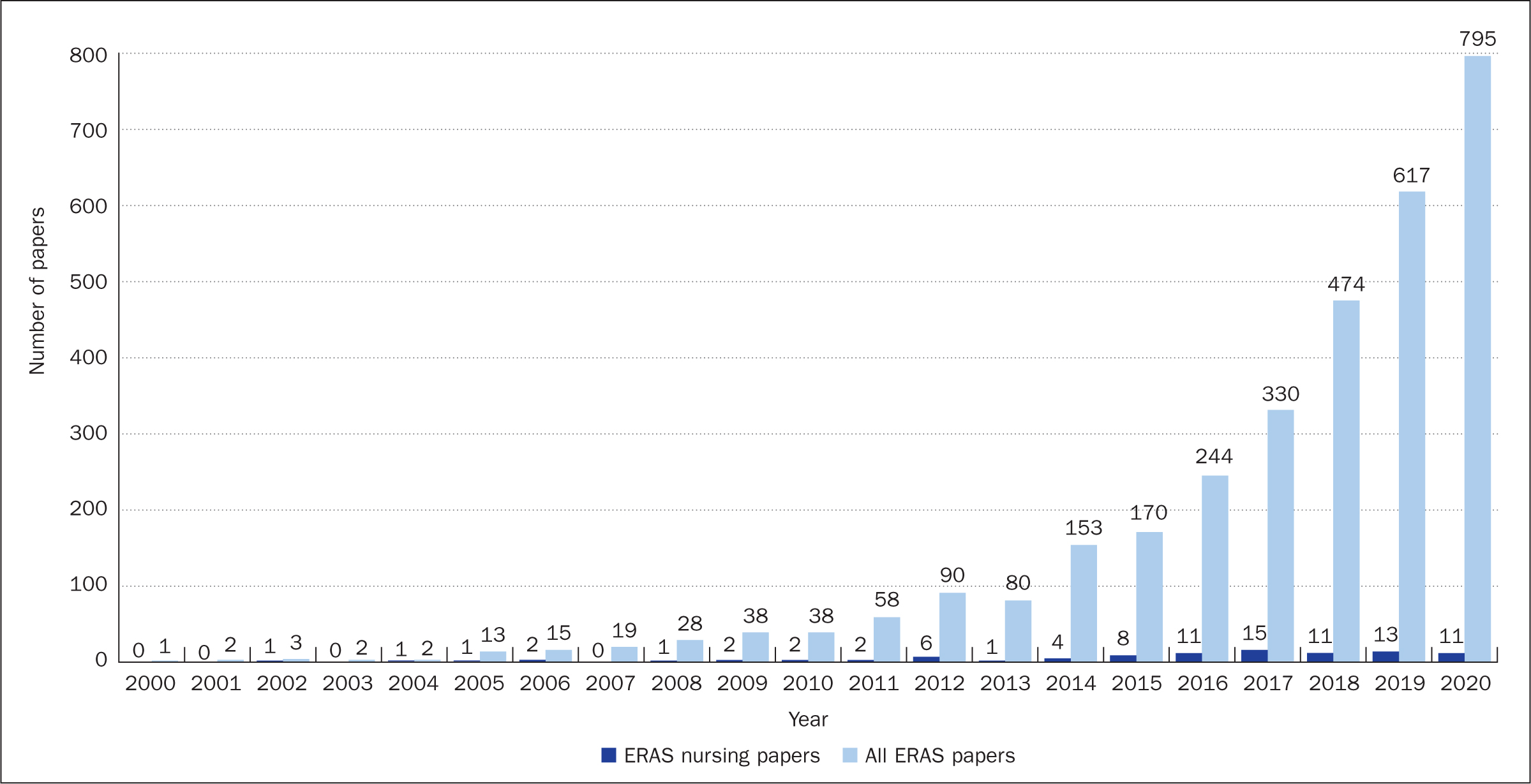
The relative low adherence to ward-based elements of ERAS pathways that are delivered by nurses is echoed by the relatively low level of nursing-specific research within the ERAS field. Until the end of 2020, there were 3278 published articles in the PubMed database that draw attention to ERAS or fast-track surgery. However, when ERAS search terms were combined with the nursing MeSH term, just 94 articles were yielded (Figure 1). Nurses, while widely recognised as being central to the ERAS concept, therefore face a challenge to not only improve the implementation of ERAS pathways but also to contribute to future research that will further improve patient care.
This article will summarise the current role of nurses within ERAS and their possible future roles, and highlight recommendations for future research within ERAS.
Current role of nurses
The ERAS concept is based on close interdisciplinary collaboration between surgeons, anaesthesiologists, nurses and allied health professionals. Each profession has its specific tasks and an essential role in contributing to compliance and sustainability of the evidence-based clinical guidelines.
Generally, nurses are the professionals who spend the most time with the patients and therefore have a vital role in implementing and maintaining ERAS programmes. Furthermore, they are often in charge of co-ordinating activities across the various professional groups involved and ensuring continuity of care. For the implementation of ERAS to be successful, nurses are vital to providing preoperative education and perioperative care and facilitating post-discharge pathways, as well as coordinating the collection of outcome measures (Brady et al, 2015).
Nurses provide the fundamentals of care such as: giving information to patients and their families; motivating and involving patients as active participants within their treatment; helping to ensure early nutrition and mobilisation following surgery; and aiding patients to prepare for discharge and rehabilitation at home. They are also essential to ensure effective pain treatment and discontinuation of invasive equipment as early as possible to enable early and intensified mobilisation and have a vital role in the monitoring and management of postoperative pain (Balfour et al, 2019).
There are three main categories of nurses, all of which have important functions in terms of achieving a successful ERAS course. The largest group are the frontline staff, who are the ones with the daily (24/7) contact and care of the patients. The second significant nursing group is the ERAS nurses, whose specific role is to facilitate the ERAS programme, focusing on compliance and clinical audit of ERAS data, staff education, patient and staff support throughout the ERAS pathway, postoperative patient support and project management (Watson, 2017; Balfour et al, 2019). The third essential group is the nursing leaders, whose role is to create the right environment needed for the ERAS concept, such as organisational initiatives, employing and securing the right nurses so that the required staff:patient ratio and skill mix are achieved, as well as offering career progression opportunities for staff, supporting the development of evidence-based care and creating a culture of safety (Brown and Xhaja, 2018).
Future role of nurses
Poor compliance with ERAS protocols in the postoperative period is a problem that needs to be addressed across all surgical procedures (Roulin et al, 2017; Aarts et al, 2018; Kehlet, 2018) and it has been shown that good adherence to ERAS protocols is significantly associated with improved clinical outcomes (Gustafsson et al, 2011).
One solution is to ensure highly trained nurses are involved. Aiken et al (2014) showed that nurse education as well as better patient:nurse ratios were significantly related to lower mortality rates. Thus, highly qualified nurses are a prerequisite for a successful ERAS patient course, and continual staff training is required to secure the best possible ERAS implementation (Francis et al, 2018).
Motivation and behaviour change are achieved primarily through gaining an understanding of the reasons why ERAS makes a major difference to the patient's recovery. A thorough introduction to the evidence behind ERAS programmes as well as their results are required. Frontline staff should be prioritised and qualified as they have close patient contact throughout the day so have the greatest impact on care. However, a basic introduction to ERAS principles and evidence is still not sufficiently provided within pre-registration educational curricula for nurses and allied health professionals.
It has been shown that in certain types of relatively uncomplicated surgery, nurses may be allowed to take over tasks from surgeons in the postoperative period, for example in total hip and knee arthroplasty, where nurses have taken over responsibility for pain management, mobilisation and discharge (Specht et al, 2015). However, this requires a well-defined care programme with clear discharge criteria and highly qualified nurses to manage the tasks. In addition, an explicit agreement on nursing roles and responsibilities will be required from surgeons that is based upon a well-defined care structure and indications for when clinical decision making should be escalated (Specht et al, 2015).
As a consequence of shorter hospital stays, nurse-led outpatient clinics for follow-up and support for patients after discharge will become more widespread in the future. As an example, a short hospital stay after breast cancer surgery can achieve the same high patient satisfaction as a traditionally significantly longer hospital stay (Carli et al, 2020). This may be achieved by introducing a nurse-led clinic where physical issues and psychosocial care are been taken care of (Duriaud et al, 2018).
In addition to the above-mentioned examples of the efficiency and task changes for the nurses, they will also have an important role in identifying and focusing on patients whose frailty and/or comorbidities may mean the standard ERAS pathway has to be adapted. Resources and interdisciplinary efforts are needed to ensure the best possible recovery for this vulnerable group of patients, with ERAS principles applied in a way that patients' individual needs are considered.
Therefore, future surgical nursing care will be divided into same-day surgery, short hospitalisations and longer hospital stay for patients with special needs. This requires surgical ERAS nurses to be trained to a high level in ERAS pathways.
Recommendations for future research
Fast-track surgery or enhanced recovery programmes have three phases: preoperative; intraoperative; and postoperative. More focus should be placed on the concept of prehabilitation, although the recent literature is a little disappointing (Carli et al, 2020) probably because outcomes have been assessed as a general composite, not with regard to outcomes that could potentially be improved by prehabilitation (Kehlet, 2021). Future research should also focus on further development of intra- and postoperative items of ERAS protocols and where implementation of evidence-based factors needs to be improved (Kehlet, 2018).
Specifically, future studies should focus on optimal intra- and early postoperative haemodynamic management, opioid-sparing multimodal analgesic strategies (Joshi and Kehlet, 2019), early mobilisation and oral nutrition, where nursing care is crucial. More research is needed regarding compliance with and sustainability of the evidence-based clinical guidelines, such as studies that include benchmarking, knowledge sharing and learning from the best.
This research should relate to not only the clinical content of the ERAS programme but also enabling organisational and cultural factors, as how care is organised and delivered is important. Examples include understanding how daily tasks are planned, the nurse:bed ratio during the daytime, evening and night, and the organisation of preoperative information and postoperative follow-up. A supportive organisational culture, continuous teaching of the evidence behind the ERAS principles, and a focus on data and outcome are essential.
So far, ERAS principles have mostly addressed early recovery, ie length of hospital stay. The focus needs to move to post-discharge recovery, which has been the subject of limited research (Kehlet, 2020). In this context, a major issue will be the potential difference between patient-reported outcomes and objective measurement of functional abilities (Kehlet, 2020).
In addition, more detailed studies are needed about different patient groups such as high-pain responders (pain catastrophisers and preoperative opioid users) and high versus low inflammatory responders (Kehlet, 2020). The intensity of the postoperative inflammatory response seems to be related to delayed recovery, but there is a large variation between individuals (Gaudillière et al, 2014). Furthermore, with regards to post-discharge rehabilitation, a distinction needs to be made between different patient groups such as those who want to continue postoperative sports activities versus the very frail, malnourished participants with reduced muscular function, as well as consideration of those who may not have specific needs or wishes for their functional recovery.
Experience from implementation of ERAS programmes over the past 25 years has shown that well-described care programmes with detailed daily goals for care are of major importance for both implementation and maintenance. Future nursing research should therefore specifically address compliance with the ERAS programmes in relation to outcomes such as complications and length of stay. An essential area of research is optimising post-discharge recovery and care through asking patients about their needs.
There is still a lack of research on nursing culture although data on care outcomes is available. Experience with audit data for use in quality development has proven to be effective and motivating for nurses to change behaviour (Jakobsen and Kehlet, 2020). Routine audit of patient recovery should be carried out to ensure optimal care quality is maintained as well as to serve as a basis for future nursing research.
Summary
ERAS is a multimodal, team-based approach where nurses are recognised as having vital caring, co-ordinating and leadership roles. However, despite this well-established and recognised role, nursing involvement within ERAS research has been limited to date.
This article highlights that improvements to nursing-related ERAS care components are possible, and that there are exciting opportunities for developing new roles for nurses within future ERAS pathways. What is clear is that as the process of developing and improving ERAS continues, nurses will need to take a major role in the preoperative clinic, in the early postoperative phase and in the follow-up, post-discharge period where the real benefits of ERAS need to be further documented. To do this, future nursing research in these areas and the subsequent dissemination of practice development must be encouraged and championed.
KEY POINTS
- Enhanced recovery after surgery (ERAS) pathways improve postoperative recovery, and reduce length of hospital stay and surgical complications
- Nurses play a vital role in ERAS pathways, are the professionals who spend the most time with patients throughout the perioperative pathway, and frequently lead and co-ordinate care across disciplines and ensure continuity of care
- Improvements are still needed, especially in the postoperative ERAS components delivered by nurses such as early mobilisation and oral feeding
- There is a paucity of ERAS nursing research. Providing opportunities for nurses and increasing nursing involvement in future ERAS research is vital to improve care and further develop and promote nursing roles
CPD reflective questions
- What are the opportunities for improvement in surgical pathways in your hospital?
- How do your surgical outcomes compare to those in exemplar Enhanced Recovery After Surgery (ERAS) centres?
- What prevents patients in your hospital from achieving discharge criteria sooner?
- How can you improve the nursing elements of your ERAS pathway?