

In Scotland, the majority of trainee advanced nurse practitioners (ANPs) are registered nurses undertaking postgraduate education through a collaborative pathway between employer and a higher education institute. Core modules undertaken often include advanced patient history taking and clinical examinations, work-based learning and independent non-medical prescribing to achieve a minimum requirement of a Postgraduate Diploma in Advanced Practice. Some are working towards a Master's in Advanced Practice. The majority of the nursing team in Hospital at Night (H@N) services are recruited as trainees in the first instance, and the service will support them to the role of ANP.
Montgomery et al (2021) acknowledged the challenges of supporting staff to undertake training in the out-of-hours period. Despite a real willingness to learn, Haslam (2021) argued that lack of access to clinical support and supervision remains the most significant barrier. Similar to the findings from other clinical environments, it would appear that the majority of clinical supervision for advanced practice comes from medical colleagues (Guevara et al, 2020; Mundy and Pow, 2021; Lee et al, 2023). This model for supervision is particularly problematic for trainee ANPs in a H@N context for a number of reasons. These include the high volume of trainees needing support against a low number of experienced ANPs; rotating medical colleagues meaning supervision is often ad hoc with little consistency; and medical consultants working during the ‘in hours’ period. This results in ANP trainees doing much of the necessary learning in their own time, outside working hours.
The introduction of a clinical practice facilitator (CPF) role is one way of addressing these issues. Within one Scottish NHS health board, this role has been developed by the authors as one whole-time equivalent. The CPFs are experienced ANPs who have undergone additional training in coaching and supervision. The CPFs more recently have also taken on the role of designated prescribing practitioner (DPP), which specifically caters for the non-medical prescribing component. This has been possible because of wider organisational investment and protected time given by the team's clinical nurse manager. The H@N team work across three acute hospital sites.
Aim
Clinical supervision for trainee ANPs has been acknowledged to be problematic for a variety of reasons. Given the rapid growth in advanced practice, there is increasing opportunity for a multiprofessional approach to supporting and supervising trainees. The aim of this small study was to explore the experiences and perceptions of those who have had or are currently receiving support and supervision from the CPFs. It is hoped that the findings will add to current understanding and offer further recommendations for advanced practice clinical supervision.
Method
Given the non-experimental nature of the study, a descriptive questionnaire was deemed appropriate (Parahoo, 2014). The questionnaire was developed to establish first, where the students were on a collaborative ANP programme and their overall satisfaction level. More specifically, the questionnaire then sought to identify where their main support had come from following the introduction of the CPF role. Two optional questions were included where participants could expand on perceived benefits and challenges of the role. The content of the questionnaire was reviewed by five experienced ANPs in the team as a means of addressing content validity (Parahoo, 2014). Purposive sampling was undertaken whereby the questionnaire was sent using the hospital's internal mailing system to the 22 eligible participants who met the inclusion criteria of the study, over a 2-month period. A participant information sheet clearly stated the aims of the evaluation and that its purpose was not to measure individual performance. Braun and Clark's (2022) thematic analysis framework was used for interpretation of the qualitative data.
Ethical considerations
A research ethics committee review was not required for this work because participants were recruited by virtue of their professional role. The Health Research Authority (2017) decision tool was used to support this work as a service evaluation not requiring formal NHS research and development ethics approval. The CPFs were granted permission through their local NHS department management team to undertake this service evaluation.
Findings
Of the 22 questionnaires distributed, 16 were returned. There was a fairly even spread of those at the early stages of the programme and those who had recently completed it. Reassuringly, from a service perspective, the majority of participants reported a very good or good experience of being a trainee and all participants reported feeling supported to undertake the programme.
Table 1 demonstrates the positive impact the CPF role has had for the respondents with 15 out of 16 identifying a CPF as one of their main sources of support. The data are also important in demonstrating the value of a multiprofessional and team-based approach to clinical supervision.
Table 1. Source of main support for trainee advanced nurse practitioners engaging with the advanced practice course
| Main source of support* | Number |
|---|---|
| Hospital at Night (H@N) clinical practice facilitator | 2 |
| Medical colleagues | 1 |
| Medical colleagues, H@N clinical practice facilitator | 1 |
| Medical colleagues, H@N clinical practice facilitator, consultant clinical leads, nursing colleagues | 3 |
| Medical colleagues, H@N clinical practice facilitator, nursing colleagues | 5 |
| Nursing colleagues, H@N clinical practice facilitator | 4 |
| Total | 16 |
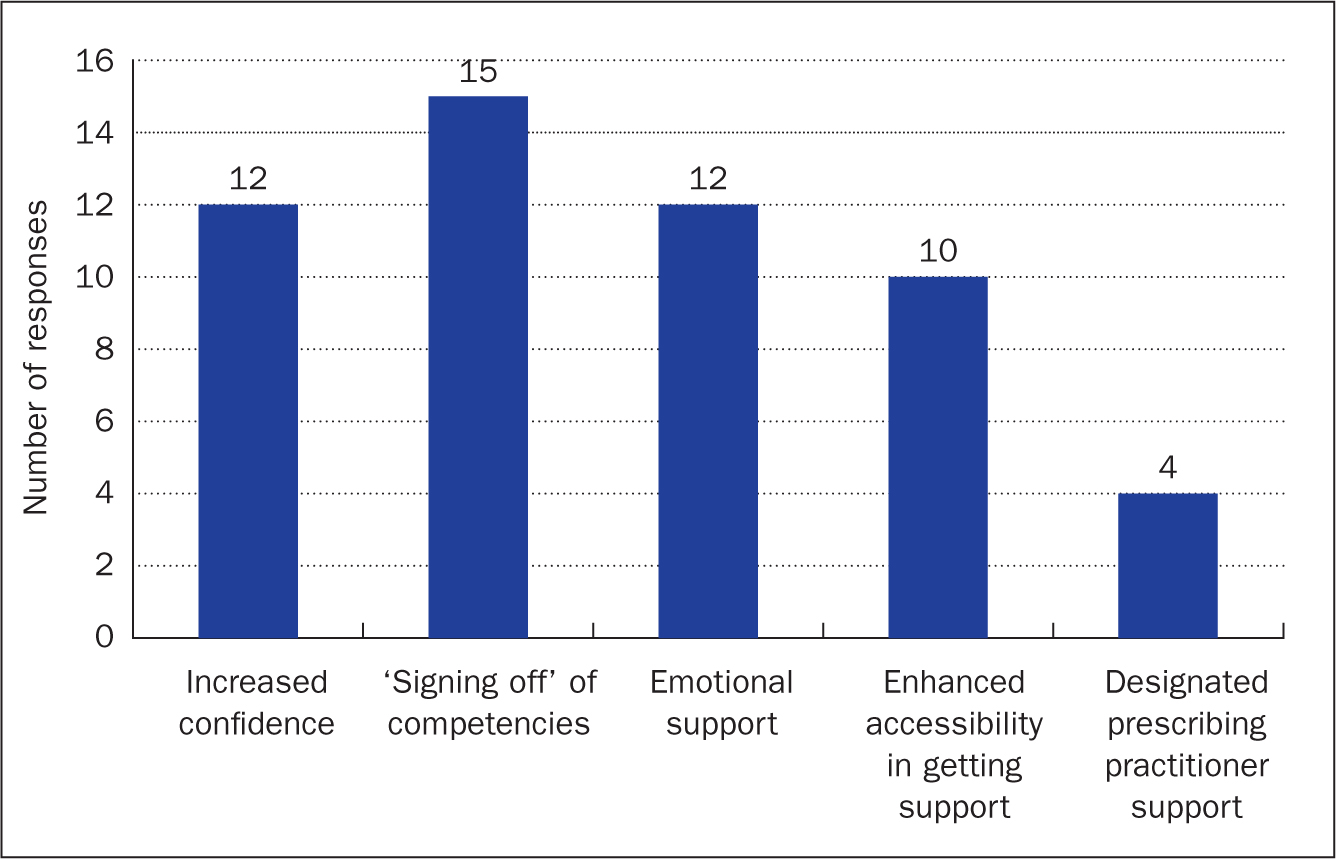
Looking more specifically at the perceived benefits of having a CPF, displayed in Figure 1, it appears from the findings that most (15/16) rated the signing off of competencies as an important aspect of the role. Increasing trainees' confidence and emotional support were also rated highly in the responses.
Two of the questions asked participants to provide free-text comments on their experiences and expectations of working with the CPFs. This textual data was analysed thematically and the following themes were developed: validation of competencies, supporting wellbeing, accessibility to a supportive source, DPP role and support post qualification. Verbatim extracts provide rich accounts of several participants' experiences.
Validation of competencies
Comments on the validation of competencies were as follows:
‘Signing off competencies is an important part of the assessment and can be done during shift whilst at work.’
Participant 3
‘The CPF has guided me with competencies and how these are signed-off.’
Participant 16
‘Non-judgemental feedback on competencies during the shift.’
Participant 6
Given that a significant proportion of the academic assessment comes from the ‘signing off’ of competencies it is not surprising that validation of these rated highest. Looking more specifically at the signing off of competencies, it is noted that having these done during allocated working hours rated favourably. Consistency and content of feedback during clinical working time was highlighted as one of the main positive outcomes noted by almost all of the participants.
Supporting wellbeing
The following comments highlighted the importance of supporting wellbeing:
‘Really helped relieve the added stress of the course.’
Participant 5
‘A huge support clinically and emotionally.’
Participant 4
The restorative component of the role became more apparent through analysis of the qualitative data. Acknowledgement of the pastoral care needed made students feel supported to engage in the learning and avoided unnecessary attrition.
Accessibility to a supportive source
The trainee ANPs made the following comments:
‘Having a “go to team” was great.’
Participant 5
‘Accessible 1:1 time.’
Participant 7
‘Taking my place in the clinical team to allow me to be available to work with medical staff.’
Participant 2
‘Happy to cover you so you can go away and do competencies, which makes a massive difference.’
Participant 9
‘The fact that they come and work with you on your nights means that you don't have to come [in] on your days off.’
Participant 13
Including a CPF role in the H@N team enables students to have someone present on shift to support training in real time. Support may come in a variety of ways, ranging from peer observation and direct feedback of practice to the facilitation of releasing them to work with other specialists.
Designated prescribing practitioner role
The trainees emphasised the importance of having a CPF with a DPP qualification, as this comment suggests:
‘[I] feel very supported to make prescribing decisions when I am being supervised by the facilitator.’
Participant 11
The DPP component relates only to students undertaking or having completed the non-medical prescribing module. This is also a relatively new aspect of the role that in the past was undertaken solely by medical colleagues within the team. It is anticipated that demand will grow as more students in the team have the CPF as their DPP.
Support post-qualification
The trainees also made the following comments about their work post qualification:
‘I would appreciate the chance to have the occasional supported shift on the wards with a clinical facilitator, as self-doubt and imposter syndrome are still the enemy of most of us!’
Participant 6
‘Once qualified as an ANP, supervised practice to ensure we are keeping up to date with current practices.’
Participant 9
A number of participants highlighted the vulnerability they feel as a newly qualified ANP. Due to the high volume of trainees in the team and prioritisation of these in the use of CPF time, the CPFs have minimal time to spend with newly qualified ANPs. The findings suggest more work needs to be done to support those in the transition from student to qualified ANP.
Discussion
It should be noted that trainee ANPs in our H@N team are not supernumerary in their clinical practice. This may strengthen the argument for the presence of the CPF not only to work directly with trainees but also to provide the flexibility to indirectly support learning. The supernumerary status and ability of the CPF to work with trainees on their shift is reflected in the notable number of participants who rated this as a significant benefit.
It was not a surprise that validation of competency rated highest in the findings, given the heavy emphasis placed on this within healthcare education. Oermann (2023) defined competency as the observable ability of the student. Competencies should align with the needs of the patient and healthcare setting (Pergert et al, 2016). Although competency rated highly within the quantitative data it is of note that the restorative component of the CPF role was consistently highlighted in the qualitative findings. The importance of this as a supportive mechanism to promote the individual health and wellbeing of staff engaging in continuing professional development is not a new concept and has been highlighted in earlier studies (Bifarin and Stonehouse, 2017; Lannan, 2017).
Until recently, there has been no consensus on the meaning and practical application of clinical supervision. In response to this, Pollock et al (2017) attempted to define clinical supervision as the provision of support and learning for healthcare practitioners to enable them to provide safe and competent practice in what may be stressful situations. NHS Education for Scotland (NES)(2021) states that there are three core components of clinical supervision: practice, restorative and professional. The CPFs are ideally placed to provide practice supervision through direct observation, discussion, clinical teaching and reflection with the trainee. The CPFs also offer restorative and professional supervision to trainees within the team.
In relation to the DPP aspect of the role, the Royal Pharmaceutical Society's (RPS) (2019)A Competency Framework for Designated Prescribing Practitioners is one example of the governance in place for the CPF to provide professional supervision, with a focus on professional competence, regulatory requirements and supporting knowledge into practice.
Taking account of a wider UK perspective, Health Education England (HEE) (2023) has recently set out explicit standards for advanced practice workplace supervision in England, including its mandatory requirement, having a named person prior to commencing training and a minimum of 1 hour of scheduled supervision every week for every trainee. The heavy investment to establish a national Centre for Advancing Practice within NHS England has not been replicated in Scotland, which has instead focused on the creation of regional Advanced Practice Academies (Kindness et al, 2019). From the authors' experiences thus far, the supervision needs of trainees have been highly variable and we would argue that addressing equitability has been more of a concern than enforcing mandatory supervision sessions. Equally, the move towards supporting and supervising via digital platforms continues to grow in popularity. NES (2021) suggested that this can be as effective as in-person sessions and may also enhance inclusivity and issues around work/life balance in those who have been hard to reach. Having time that is planned and protected has been pivotal to successful implementation of the CPF role. This has necessitated not only commitment from a professional level but also support given by the wider management team.
The focus here has been on the experiences of trainees within one advanced practice team. The findings have also highlighted some of the vulnerabilities and deficits in support that newly qualified ANPs may experience. There is a growing body of literature on the transition from trainee to qualified advanced practitioner (Murphy and Mortimore, 2020; Reynolds and Mortimore, 2021; Fothergill et al 2022). Given the heavy investment currently in place to support trainee ANPs, further research should focus on the importance of the clinical environment and how best to implement a standardised approach as advocated by HEE (2023) and NES (2021).
Study limitations
This study reflects the experiences of participants in one service across three acute hospital sites in one health board in Scotland. Therefore, the results may not be generalisable. It may, however, have some relevance, both nationally and internationally, for other trainee and qualified ANPs. The study focuses entirely on those who are currently being supported or recently supported by the CPFs.
The primary investigators were the CPFs themselves, albeit the first author is now seconded as a teaching fellow outside of clinical practice. The insider familiarity and awareness of both advanced practice and clinical supervision enabled a distinct recognition of the study participants' context and experience. It should be acknowledged that because the participants were known to the investigators this could have affected the participants' responses. It should be stressed that all participants were encouraged to be candid in their responses and reminded that it was not intended as a measure of individual performance but instead as a service evaluation. Awareness that this was a small group of participants meant that basic demographics such as age and gender were not obtained to help preserve anonymity. Participants were recruited on a voluntary basis whereby a group email was sent to the 22 selected participants.
Reflective processing, as described by Bassot (2016), through self-monitoring and journal writing, was undertaken throughout the evaluation in a conscious effort to handle biases or assumptions. Thematic analysis was subject to external input from an experienced university researcher to mitigate any further concerns surrounding bias. Content validity for the questionnaire was sought from experienced ANPs in the team.
Conclusion and recommendations
This evaluation has described the positive benefits of integrating the CPF role in a H@N service, particularly in relation to accessibility to appropriate clinical supervision. It is both a professional and organisational responsibilty to ensure that practitioners have access to adequate supervision whatever stage they are at. The findings of this study stress the importance of acknowledging the restorative component of clinical supervision.
As experienced advanced practitioners with additional training invested in coaching and clinical supervision, CPFs are ideally placed to meet the training needs and provide support to those on advanced practice diploma and masters' programmes. CPFs have the advantage of combining advanced clinical knowledge with the practical application of also being able to work flexibly alongside trainees in the various practice areas. As the landscape of the healthcare workforce continues to diversify, it is vital that developments in advanced practice are not solely reliant on our medical colleagues to drive quality and standards. Notwithstanding issues around sustainability, ongoing organisational commitment is key to ensuring ANPs are in optimal positions to provide support and supervision for the next generation of trainees.
KEY POINTS
- This evaluative study describes trainee advanced nurse practitioners' experiences and perceptions of having a clinical practice facilitator introduced into their team
- The challenges of providing adequate clinical supervision, particularly in the out-of-hours period, or in teams with high training demands, have been acknowledged
- Organisational investment, together with professional development, is needed to deliver high-quality multiprofessional clinical supervision
- Clinical supervision that is not solely dependent on one professional group is key to sustainability and improving current practices
- Having dedicated and protected time within the clinical area optimises opportunities for effective workplace supervision
CPD reflective questions
- What has your experience been of clinical supervision for advanced practitioners in your workplace?
- Do you have access to constant supervision? How is this monitored and supported?
- This study highlights the importance of a multiprofessional approach with protected and dedicated time. How can you influence or enhance clinical supervision in your workplace?
- How might a clinical practice facilitator role be positively implemented within your own workplace?