

It is estimated that there are more than 205 000 ostomates living in the UK (Marinova et al, 2021), and around 600 stoma nurses, which means there is an average nurse to patient ratio of around 1 to 342. The availability of stoma nurse specialists and long-term support may differ between locations, as some areas may have more stoma nurse specialists than others, so the ratio will vary.
Having a colostomy can have a significant psychosocial impact on patients (Dabirian et al, 2010; Anaraki et al, 2012; Boutry et al, 2021) and these individuals may benefit from interventions intended to improve their quality of life (QoL).
Patients with a colostomy may be able to perform colostomy irrigation, which may improve their QoL and help them achieve a degree of bowel control for a period of 24–72 hours (Hayes, 2013; Cobb et al, 2015; Kent et al, 2015, Boutry et al, 2021; Jones, 2021).
Colostomy irrigation
Colostomy irrigation is a procedure that involves introducing water into the large intestine through the colostomy opening to help empty the bowel. It requires the instillation of 500-1000 ml of body-temperature water (37°C); the water then distends the intestine causing wave-like motions (peristalsis), which expel stool and flatus (wind) from the large intestine (Figure 1).
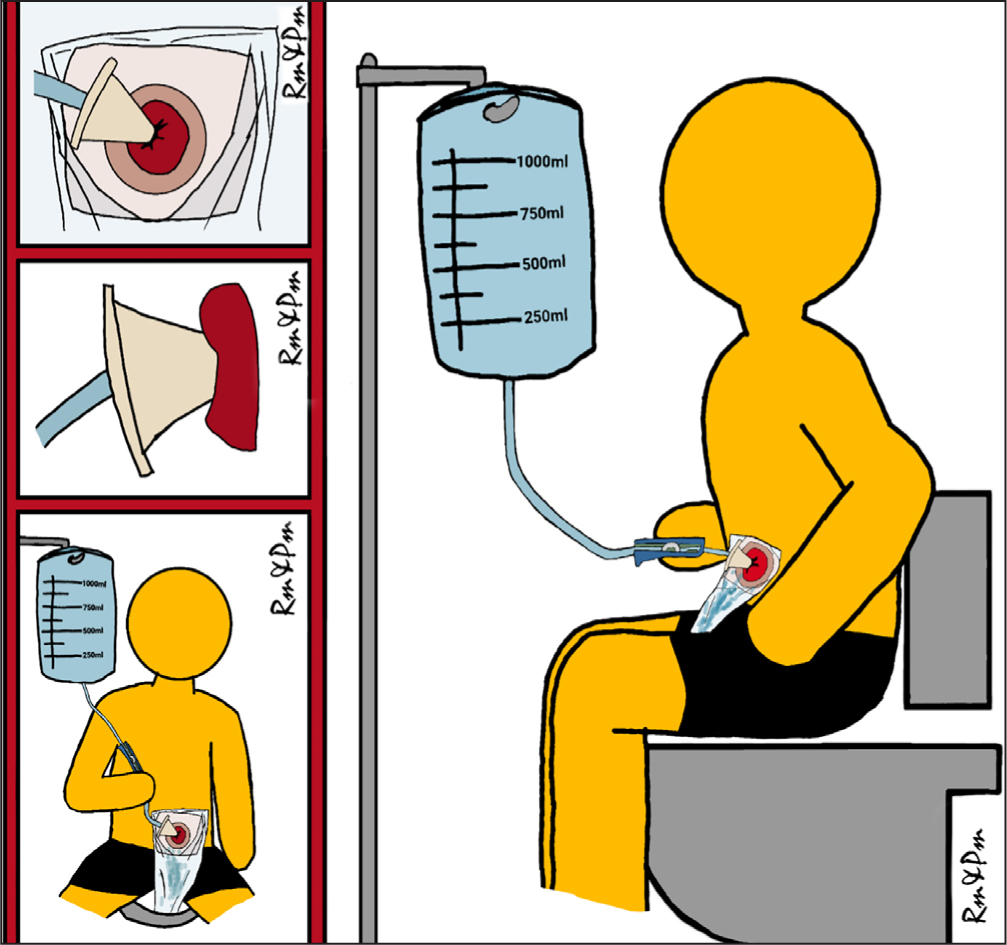
The procedure requires: an irrigation kit or irrigation pump, which contains a soft cone; flexible tubing equipped with a flow regulation valve; a water container filled with water; and an irrigation sleeve with two openings, which is applied to the peristomal skin.
Colostomy irrigation is not suitable for all patients, and strict inclusion and exclusion criteria should be put in place to ensure the procedure is safe and not contraindicated (Woodhouse, 2005; Tallman et al, 2015).
Colostomy irrigation should generally be offered to patients with an end, descending or sigmoid colon colostomy, and the procedure is normally contraindicated in the first 2–3 months after surgery, although there are cases when it has been used earlier. Other inclusion criteria are having a lifestyle that allows the procedure to be performed, having the colorectal surgeon's consent (to eliminate any physiological contraindications), the patient being able and willing to learn, adequate personal hygiene, daily access to a toilet for prolonged periods and adequate manual dexterity (Turnbull, 2003; Hayes, 2013; Association of Stoma Care Nurses (ASCN), 2016; Marinova et al, 2021). Furthermore, various health conditions may render colostomy irrigation contraindicated. While this list is not exhaustive, these include:
- Active diverticular diseases
- Crohn's disease
- Ulcerative colitis
- Persistent diarrhoea
- Parastomal hernia
- Stomal prolapse
- Ongoing radio/chemotherapy
- Stoma stricture
- Severe cardiovascular insufficiency
- Kidney disease
- Dementia (Turnbull, 2003; Hayes, 2013; ASCN, 2016; Marinova et al, 2021).
Additionally, psychiatric conditions, difficulties in seeing the stoma, lack of motivation, cognitive impairment, visual impairment and poor manual dexterity may make colostomy irrigation difficult to achieve or even contraindicated (Karadağ et al, 2005; Hayes, 2013; Marinova et al, 2021).
Research suggests that colostomy irrigation may improve QoL and body image, and reduce anxiety, bowel frequency and stoma bag use, so it could potentially reduce costs, as well as address or eliminate stoma-related complications and issues such as peristomal skin damage, odour intensity, flatulence, dietary limits and social restrictions (Karadag et al, 2009; Carlsson et al, 2010; Grant et al, 2011; Kent et al, 2015; Boutry et al, 2021; Jones, 2021).
The advantages and disadvantages of colostomy irrigation need to be discussed with patients to ensure they have realistic expectations (Marinova et al, 2021).
The advantages of irrigation are:
- Up to 72 hours without a bowel motion between irrigations
- A level of bowel control
- Eliminates or reduces the need for a colostomy bag (a discreet stoma cap may be used)
- Reduced odour and flatus
- Improved body image and confidence
- Possible reduction in anxiety
- Possible alleviation of constipation
- May help prevent or improve peristomal skin irritation.
The disadvantages of irrigation are:
- It is time consuming: it can take up to 60 minutes or longer
- It requires uninterrupted periods of time on the toilet
- Irrigation must be continued while on holiday or abroad
- There may be unexpected stoma output between irrigations
- Colostomy bags may still be needed
- Irrigation may have to be stopped if the patient's health condition changes.
Colostomy irrigation protocol
An audit at a tertiary centre showed that colostomy irrigation was not routinely offered to patients who had undergone this procedure, an observation shared by both patients and health professionals (Woodhouse, 2005; Bowles et al, 2022).
Therefore, the authors' stoma care team decided to produce a protocol to ensure colostomy irrigation is routinely offered to suitable patients, as well as provide them with a structured follow-up.
After an extensive literature review, the authors' stoma care team formulated a colostomy irrigation protocol, ensuring that each step of the patient's colostomy irrigation journey is captured and actions are put in place to provide excellent care. To test the efficacy of the protocol, it was piloted and trialled with two colostomy irrigation patients. Their case studies are given below.
Strict inclusion and exclusion criteria were drawn up in line with national and international recommendations, ensuring that only suitable candidates are offered colostomy irrigation, which helps ensure a seamless service for both patients and clinicians.
To ensure that no colostomy patients were discriminated against and excluded from being offered the procedure, the authors' colostomy irrigation protocol states that stoma nurses may discuss colostomy irrigations with suitable candidates at any stage of their journey with a colostomy. This could be preoperatively and after surgery while in hospital, as well as when patients have had their stoma for at least 2-3 months.
Once a suitable candidate is identified, the protocol requires confirmation of safety and consent from the patient's colorectal surgeon before starting the procedure. This is to ensure that patient safety is maintained, taking into account any surgical contraindications, which is in line with national and international guidelines (ASCN, 2016; Marinova et al, 2021).
Only after the safety of the procedure has been confirmed and the patient is happy to proceed is training arranged. This is normally provided in hospital because of the known risk of vasovagal reaction with colostomy irrigation, in particular during the initial procedure(s). During this training session, the Stoma-QoL questionnaire (Prieto et al, 2005) is administered to provide a baseline QoL. This will help the team monitor how effective colostomy irrigation has been in improving QoL (Box 1).
Box 1.
Process at colostomy irrigation training session
- Complete Stoma-Quality of Life questionnaire (Prieto et al, 2005)
- Demonstrate procedure and encourage the patient to participate
- Provide colostomy irrigation patient passport and irrigation starter kit
- If further training required, arrange training 1 or 2 more days' training
The Stoma-QoL questionnaire was chosen because it was created and validated specifically to measure the QoL of stoma patients (Prieto et al, 2005). The 20 questions are distributed in the following categories of problems related to: sleep; intimate relationships; relationships with family and close friends; and relationships with people outside the family. The answers are based on a four-point Likert scale (1=always; 2=sometimes; 3=rarely; 4=not at all). One answer must be provided for each question and all 20 questions must be answered for the result to be valid. The minimum score is 20 and the maximum is 80. The higher the score, the better the QoL. The authors added a field to the questionnaire to indicate during which session or follow-up appointment it was completed.
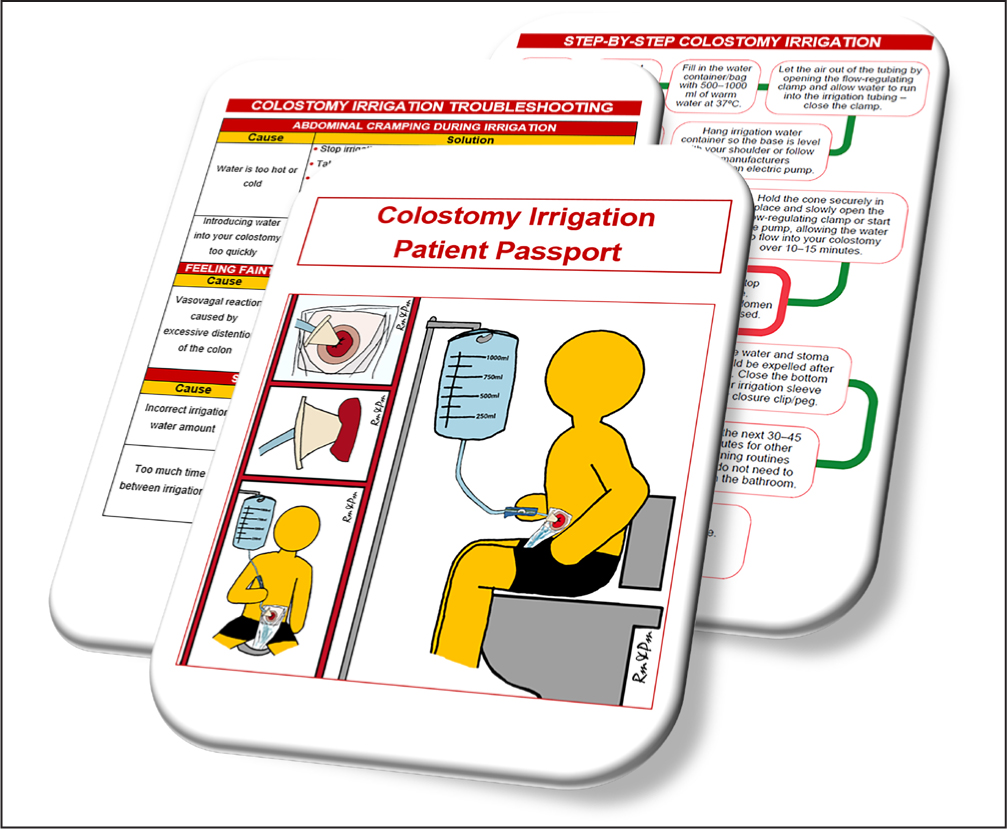
Once training has been provided and the patient deemed competent, they are given a colostomy irrigation kit and a copy of the colostomy irrigation patient passport, designed for these patients by the authors. The patient passport is a booklet with all the information the patient may need to perform colostomy irrigation at home, including step-by-step instructions, how to troubleshoot common problems associated with the procedure independently, as well as information and codes of common irrigation products, hints and tips (Figure 2).
All this is aimed at empowering patients to self-care, as well as to prevent unnecessary hospital appointments and follow-ups. If a patient is not deemed independent after the first hospital visit, they may require 1-2 additional training sessions. Failure to perform the procedure independently after 2-3 training sessions should prompt clinicians to reassess the patient and decide whether colostomy irrigation is suitable for them.
Involving carers may be an option for patients who wish to have others involved but only where appropriate, as patients' independence should be preserved. Patients should not be rendered dependent on others as colostomy irrigation is aimed at improving QoL while not taking away the individual's ability to self-care.
As part of the colostomy irrigation protocol, the authors' tertiary centre also provides patients with a structured follow-up, including clinical review at 1 week, 1 month, and then at months 3, 6 and 12 (Figure 3).
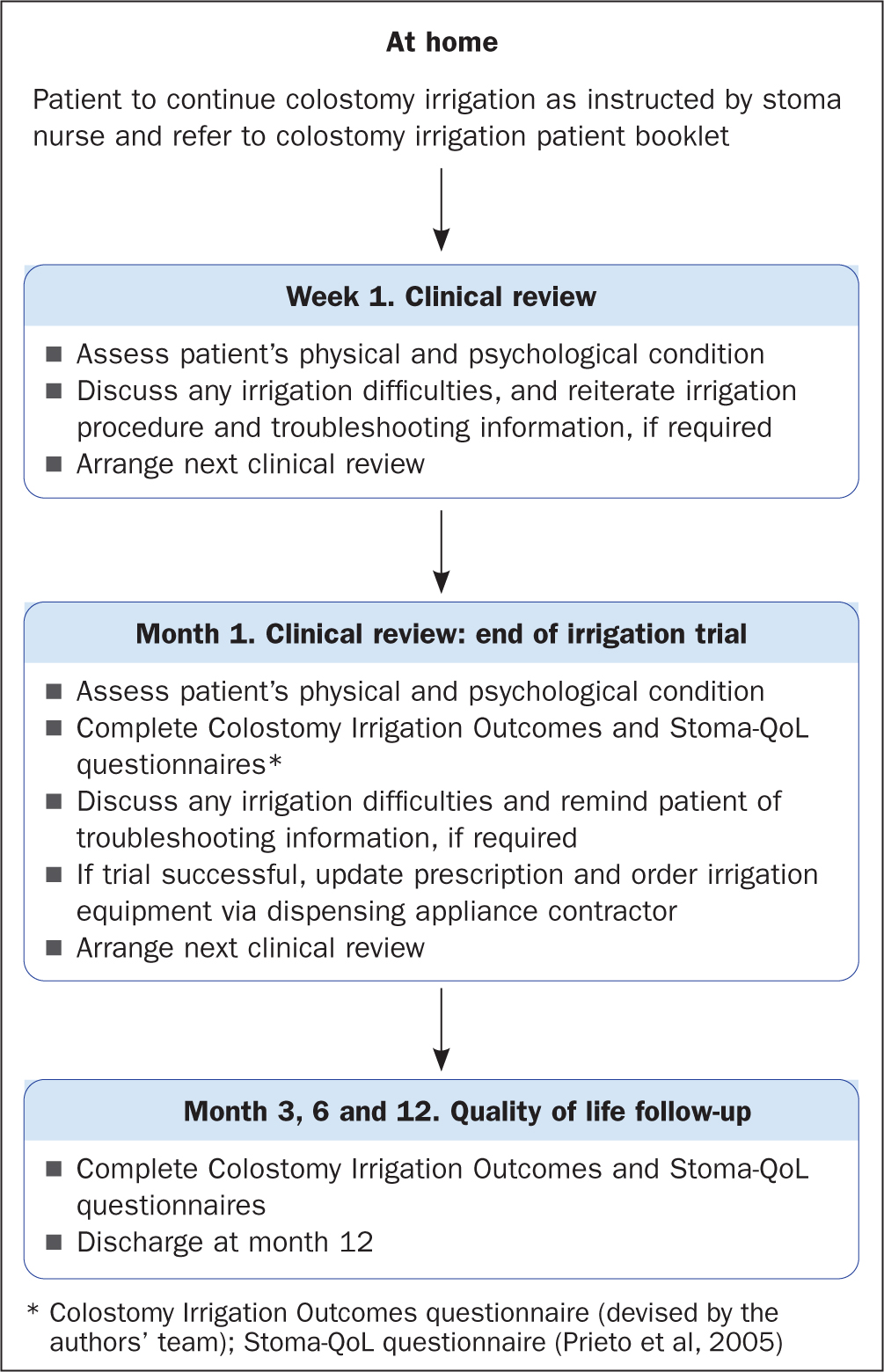
These follow-ups are aimed at ensuring a smooth transition and adjustment to colostomy irrigation, as well as reducing the risk of non-compliance because of complications and/or difficulties, because colostomy irrigation requires perseverance, especially during the first few months when patients are establishing and adapting to a new bowel routine.
To ensure that both QoL and the efficacy of colostomy irrigation are monitored, the authors' protocol requires that the Stoma-QoL questionnaire is administered at each structured clinical review, which provides insight into the patient's QoL while carrying out colostomy irrigation.
Additionally, the team has designed their own questionnaire – the Colostomy Irrigation Outcomes (CIO) questionnaire, which has been validated internally – as part of trialling the new protocol with patients. It has been formulated to help measure the efficacy and outcomes of colostomy irrigation, including how long it takes to complete irrigation and whether it helps achieve bowel control between procedures, reduce flatus, help improve QoL, reduce stoma-related problems and reduce the number of appliances used. The CIO questionnaire is administered at each structured follow-up review. (A copy of the CIO questionnaire is available on request from the authors.)
Patients are followed up for 1 year then discharged from routine follow-up, although they can access the stoma care service via telephone and/or email advice lines at any time over the 1-year period and after their discharge.
Case study 1
This patient had a colostomy after abdominoperineal excision of rectum (APER) surgery to improve QoL.
Patient history
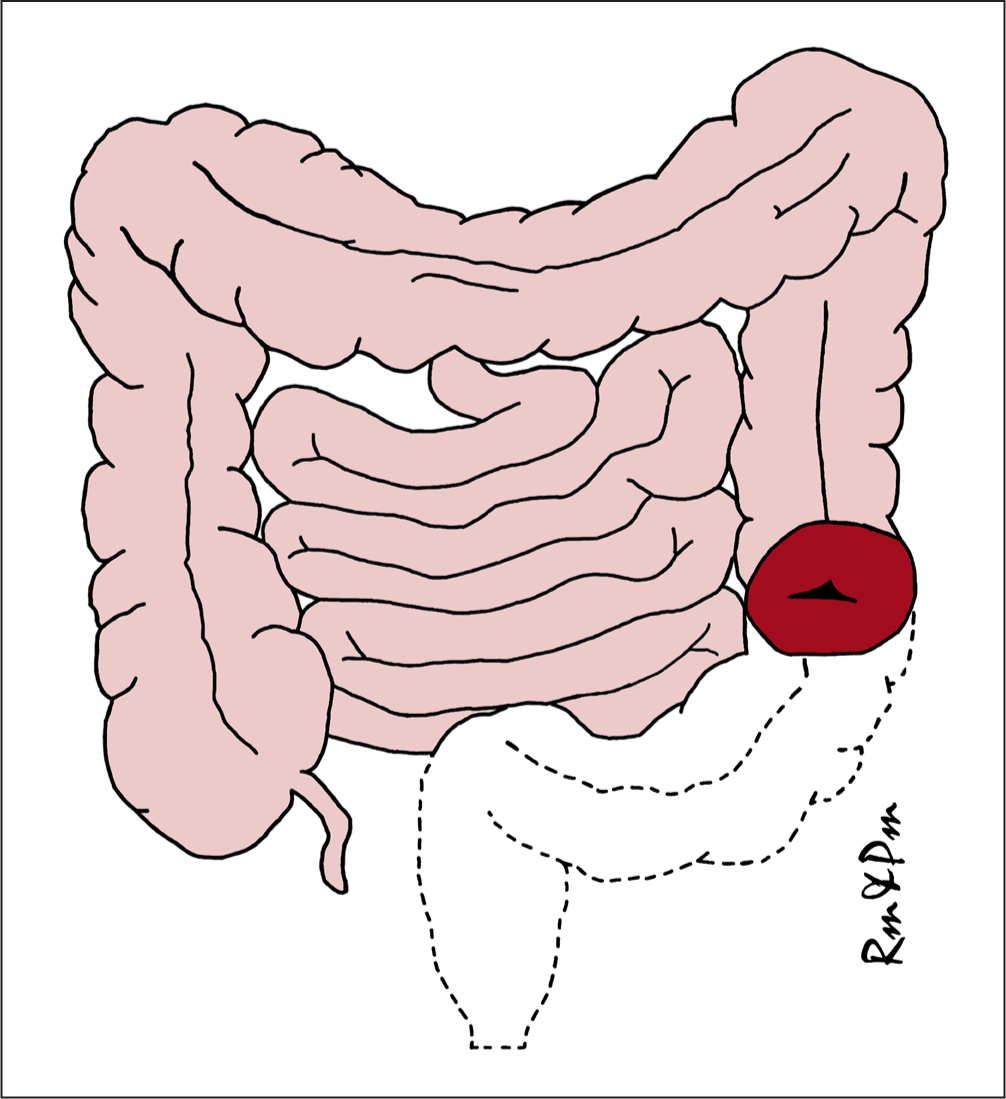
The patient is a man in his mid-fifties. Following a diagnosis of bowel cancer, he underwent APER – removal of the sigmoid colon, rectum and anus – and the formation of a permanent end colostomy (Figure 3).
Patient overview
The patient had no issues with his stoma care but wanted to trial colostomy irrigation as a way of improving his QoL and body image, as he did not feel confident meeting new people. His colostomy output was of semi-formed consistency and he changed his stoma appliance once a day using a drainable stoma bag.
Intervention
The patient was introduced to colostomy irrigation at a face-to-face clinic, where the procedure, rationale and expected outcomes were explained, as well as possible complications and troubleshooting. He decided to proceed with it.
As the patient was a suitable colostomy irrigation candidate, consent was obtained from his colorectal consultant and he was then seen in a nurse-led stoma care clinic for training in colostomy irrigation. His ability to perform the procedure was assessed in the clinic and then the procedure was performed with a stoma nurse specialist. The patient experienced some of the well-known complications while in clinic, including feeling light-headed and dizzy (a vasovagal reaction), which were managed by the stoma nurse specialist. He was given a colostomy irrigation patient passport, which included troubleshooting instructions to use if similar or other problems occurred.
A baseline QoL assessment was performed using the Stoma-QoL questionnaire (Prieto et al, 2005), where the patient scored 52/80 points, which was consistent with how he said he felt: his score was low in the sections on intimate relationships and relationships with people outside the family. He said his main concern was meeting new people due to having a stoma bag.
He was then provided with the necessary equipment, and regular follow-ups were arranged to assess his progress as well as his QoL; at 1 week after the first colostomy irrigation, then at 1 month, 3 months, 6 months and 12 months. He was able to access ad-hoc stoma nurse interventions when additional troubleshooting was required. These routine structured follow-ups were in line with the hospital's colostomy irrigation protocol.
The patient's QoL showed significant improvement after 1 month, when he scored 72/80 on the Stoma-QoL questionnaire. His QoL score then increased to 79/80 at 3 months and remained in the 78-79/80 range throughout the remaining period of the structured follow-up over 3-12 months.
During the regular structured follow-ups, he reported that, since starting colostomy irrigation, his QoL had greatly improved. He was able to meet new people, travel abroad for work and make adjustments to irrigate when in hotels, resume working out and lose weight, as well as to meet a new partner.
He was able to achieve at least 48 hours without output in his stoma appliance, with minimal (smear) to no stoma output between irrigations.
At the end of the trial, the patient was able to complete the procedure in 30-45 minutes (mean: 38 minutes), and reported improved peristomal skin health, as well as reduced flatus and odour, and using fewer stoma bags. He also felt that the time between each follow-up appointment was satisfactory.
Although the procedure was time consuming, the patient reported that he did not give up other activities to make time for this, and the time required did not make him consider abandoning irrigation, as he considered the time dedicated to completing it worth it. He said he would recommend colostomy irrigation to other colostomy patients, if asked.
Outcomes
Colostomy irrigation significantly improved this patient's QoL and allowed him to return to the life he had led before colostomy formation surgery. His body image was also greatly improved, helping him to return to meeting new people and to start a relationship with a new partner. It also reduced his use of stoma appliances and therefore expenditure on products.
Case study 2
This patient had a colostomy after pelvic exenteration surgery to improve QoL.
Patient history
The patient is a woman in her late thirties. Following a diagnosis of bowel cancer, she underwent cancer treatments and complex bowel surgeries, involving the removal of multiple pelvic organs, and resulting in the formation of a permanent colostomy.
Patient overview
The patient had no issues with her stoma care. Her colostomy output was of a semi-formed to formed consistency, and she changed her stoma appliance once a day using a closed stoma bag.
She wanted to trial colostomy irrigation as a way of improving her QoL and body image, because she did not feel confident going out with a stoma bag, fearing that it might leak. She avoided social interaction, travelling and staying away from home because of this concern. She avoided eating and drinking when outside her home, because she feared her stoma may become active, resulting in her needing to change her stoma bag while outside.
Intervention
The patient was introduced to colostomy irrigation via video consultation, where the procedure, rationale and expected outcomes were explained, as well as possible complications and how to troubleshoot them. She decided to proceed with the procedure.
Because the patient was a suitable colostomy irrigation candidate, consent was obtained from her colorectal consultant and she was then seen in a nurse-led stoma care clinic for training in colostomy irrigation, where her ability to perform the procedure was assessed. This was performed with a stoma nurse specialist.
A baseline QoL assessment was administered using the Stoma-QoL questionnaire (Prieto et al, 2005). The patient scored 27/80 points, which was a significantly poor score.
She was then provided with the necessary equipment, as well as having regular follow-ups to assess her progress and QoL at 1 week after colostomy irrigation, then at 1 month, 3 months, 6 months, and 12 months; she was offered ad-hoc stoma nurse interventions when troubleshooting was required. These routine structured follow-ups were in line with the hospital's colostomy irrigation protocol.
The patient's QoL showed significant improvement at 1 month, and her QoL remained at 68/80 from month 1 to month 6. She could not complete the 12-month Stoma-QoL questionnaire because she could not attend the follow-up because of personal circumstances.
During the regular structured follow-ups, she reported that, since starting colostomy irrigation, her QoL had greatly improved. She was able to travel, go on holiday abroad and to spend a night or weekend away from home without worrying about her stoma, as well as return to work.
She was able to achieve at least 24 hours without output in her stoma appliance, with minimal (smear) to no stoma output between irrigations, and therefore she did not need to worry about changing her stoma bag when out and about as she required only a discreet stoma cap.
At the end of the trial, the patient was able to complete the procedure in 30-45 minutes (mean: 40 minutes), she reported improved peristomal skin health, as well as reduced flatus and odour, and used fewer stoma bags. She also felt that the time between each follow-up appointment was satisfactory. Although the procedure was time consuming, the patient reported she did not need to give up other activities to make up time for irrigation; this did not make her consider abandoning irrigation, as she considered the time dedicated to carrying it out was worth it.
The patient stated that she would recommend colostomy irrigation to other colostomy patients, if asked.
Outcomes
Although the patient did not attend the 12-month follow-up, she continued to use colostomy irrigation long term, which helped significantly improve her QoL, body image, confidence and reduce anxiety. She also used fewer stoma appliances which saved money.
Limitations
This small sample of patients did not allow for a more robust collection of data, which would have provided more detailed and accurate information. Nonetheless, the team acknowledged that these patients were part of a trial to help understand the functionality of the protocol.
Considerations and resources
The case studies show that colostomy irrigation may improve QoL in patients with a colostomy. This is also in line with findings in the literature (Karadag et al, 2009; Carlsson et al, 2010; Grant et al, 2011; Kent et al, 2015; Boutry et al, 2021; Jones, 2021).
The case study outcomes showed that both patients had less anxiety, more confidence and improved body image, and used fewer stoma products.
It is important to note that colostomy irrigation requires time to carry out the procedure, as well as skilled stoma care clinicians. It requires investment in workforce and infrastructure, as training a patient may take up to 2 hours in clinic, and the entire process of pre-procedure counselling, training, structured follow-up, ad-hoc advice and troubleshooting, as well as providing and completing documentation, may require an average of 10-15 clinical hours per patient.
Therefore, it is of paramount importance to have the resources to conduct these clinics, dedicated clinical space and trained stoma nurses, as the authors' experience from patient feedback is that colostomy irrigation is not routinely offered and, when patients enquire about it, they are often referred to a tertiary centre in stoma care or denied this opportunity.
Conclusion
Colostomy irrigation should be offered routinely to suitable candidates, as it has the potential to improve QoL, body image and aspects of stoma care. The procedure should be discussed with suitable candidates in the preoperative, as well as postoperative periods.
Questionnaires such as the Stoma QoL (Prieto et al, 2005) and the authors' CIO questionnaire are helpful tools to assess the efficacy of colostomy irrigation and how it affects patients' QoL over a period of time, for example at 1, 3, 6 and 12 months. Such tools can also help practitioners to monitor patients for any problems and address them in a timely manner.
KEY POINTS
- Having a structured follow-up is essential in ensuring patients are supported and any problems with colostomy irrigation identified and resolved
- Colostomy patients should be offered colostomy irrigation to optimise their quality of life, and this should be done by specialist stoma nurses to ensure they are understood and well supported
- Colostomy irrigation is a stoma nurse specialist skill, because it requires an advanced physical and functional assessment, as well as critical thinking necessary for effective troubleshooting.
CPD reflective questions
- What are the benefits of colostomy irrigation, and why should structured protocols and follow-ups be set up?
- Are there challenges in implementing colostomy irrigation clinics in day-to-day stoma services?
- What are the cost implications of offering colostomy irrigation to patients?