

Since the 1990s advancements in antiretroviral therapy (ART) have revolutionised the medical treatment of HIV and continue to do so. Despite the care of HIV being transformed into that of a chronic manageable condition, people living with HIV experience a wide range of issues that impact on their quality of life, one of these issues being poor sleep quality and sleep disturbances (Bourne et al, 2022).
In the wider population, poor sleep has been linked to an increase in cardiovascular disease (Malhotra and Loscalzo, 2009), diabetes (Knutson et al, 2006), obesity (Beccuti and Pannain, 2011) and reduced immune function (Savard et al, 2003). Moreover, poor sleep has consistently been linked to poor mental health as people are more likely to suffer with depression and anxiety (Goldstein and Walker, 2014). as well as suicidal ideation and behaviour (Pigeon et al, 2012). Conversely, good sleep has been strongly linked to wellbeing and it is therefore essential for health professionals to understand more about this phenomenon within HIV care (Garbarino et al, 2016).
Consequently, it should cause clinicians concern that sleep disturbances have long been identified at various stages of HIV infection and disease progression (Norman et al, 1988); they have been consistently recognised as being more common in people living with HIV than in the general population, with estimated prevalence rates of between 30% and 100%, depending on definition and methodology (Rubinstein and Selwyn, 1998; Lee et al, 2012; Gutierrez et al, 2019).
In people living with HIV, sleep disturbances have been associated with an increased risk of cardiovascular disease, metabolic disease, impaired cognition, poor adherence to ART, decline in immune function and suicide (Saberi et al, 2011; Lee et al, 2012; Wu et al, 2015; Koren et al, 2016).
Despite this large body of literature, there is a lack of clinical guidance on how to screen for and treat sleep disturbances (Gutierrez et al, 2019). As the care paradigm for people living with HIV continues to evolve, healthcare providers are encouraged to incorporate quality of life issues such as sleep into routine clinical care.
A scoping review was carried out to explore how sleep is currently measured within HIV care with the aim of improving awareness of quality life issues experienced by people living with HIV. This article examines what is known from the existing literature about how sleep is measured in HIV care and explores the implications for clinical practice and research
Method
Scoping reviews aim to rapidly map the key concepts underpinning a research area, by exploring the evidence available to understand more about a particular area of research and practice. These reviews can be undertaken as a stand-alone project in their own right, especially when the area is complex or has not been previously reviewed (Mays et al, 2001). They are a popular approach to reviewing health research to inform clinical practice (Levac et al, 2010). We chose this approach because it allows for the inclusion of many different study designs, which meets with the aim of identifying what is known about how sleep is measured in HIV care.
Arksey and O'Malley (2005) suggested that there are five stages to a scoping review and that the process should be documented in sufficient detail to enable the study to be replicated by others.
Stage 1. Identify the research question
To identify the scope of the review we focused on the following research question: What is known from the existing literature about how sleep is measured in HIV care? The review aimed to examine the current available literature on how sleep is measured in HIV care and to identify issues for clinical practice, as well as any gaps in current knowledge, to help inform research priorities.
Stage 2. Identify relevant studies
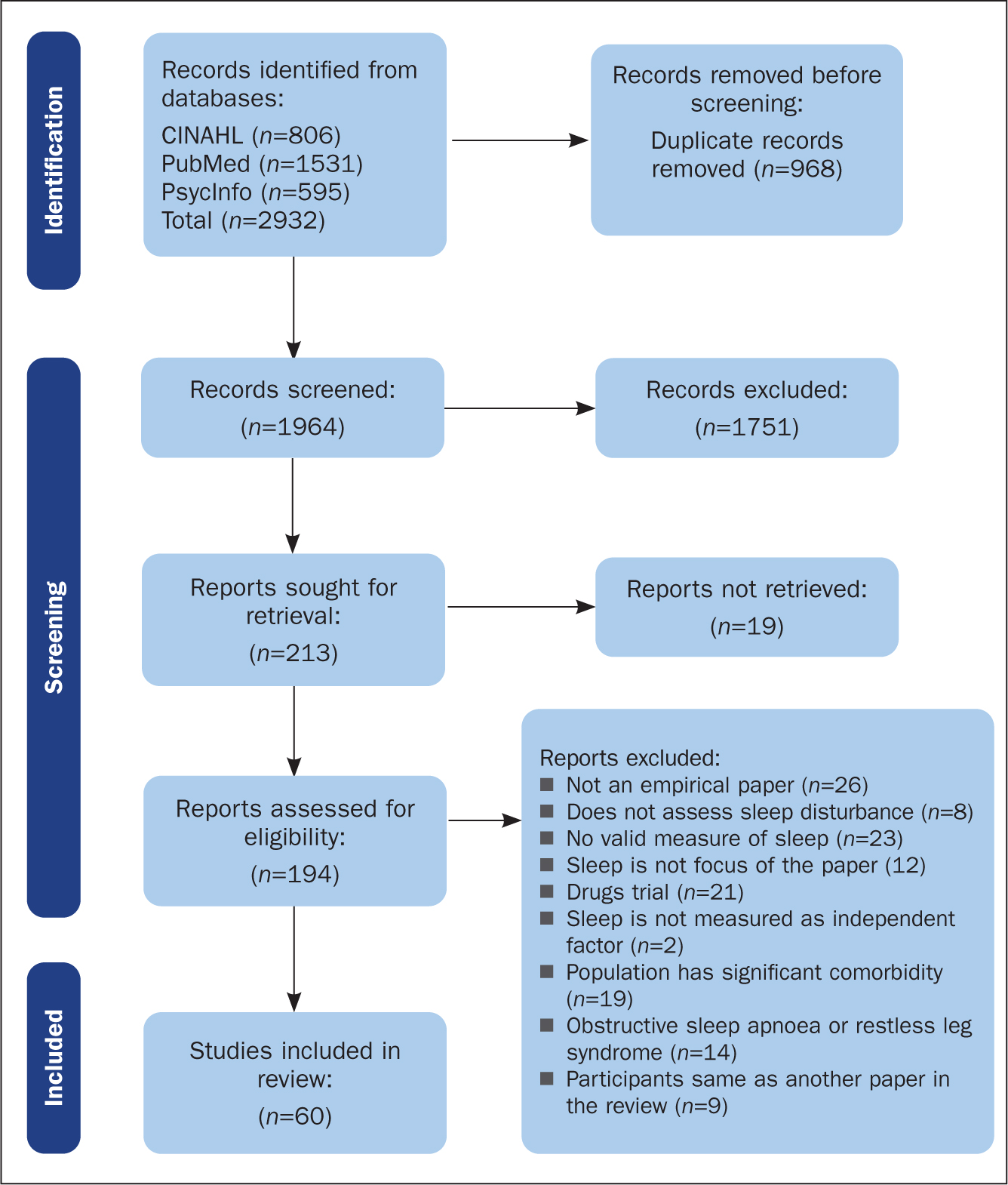
A comprehensive literature search included the databases PubMed, CINAHL and PsycInfo, which were searched from 1980 to present day, with language limited to English. Our search was limited to 1980 (when HIV was identified as an emergent health concern); as a final search step, we also hand-searched reference lists to reduce the likelihood of missing articles.
References were imported into the Zotero management system, and duplicates removed. Studies were screened at three stages. Titles were reviewed by one member of the research team. The remaining abstracts were then reviewed by two members of the team separately, with a joint review session to reach a consensus on those not included by both researchers. The full text of the remaining articles was then reviewed separately. Articles without abstracts were automatically included in the full text review stage.
Stage 3. Study selection
At each stage, a selection of 100 articles were reviewed by reviewers to reach consensus about applying the inclusion and exclusion criteria (see Figure 1). Following this each, reviewer reviewed the articles separately. At each stage of the review the articles were divided into the following categories: relevant, irrelevant and discuss. In order to ensure validity of the inclusion and exclusion criteria throughout the selection process the two reviewers regularly checked for consistency.
Stage 4. Charting the data
A data charting form was developed by the two reviewers to determine which variables to extract. The reviewers independently charted the data, discussed the results and updated the data charting form in an iterative process. The following data were extracted: date of publication, country, study design, participants, and how sleep was measured.
Stage 5. Collating, summarising and reporting
In order to explore how sleep was measured in HIV care we applied a qualitative content analysis approach (Levac et al, 2010). This resulted in the following themes emerging: range of methods available to assess sleep, self-reported sleep measure and objective measure of sleep.
Results
Table 1 lists the 60 studies included in the review. A full overview of the included studies and the data extracted (as discussed under Stage 4) is appended to the online version of this article.
Table 1. Included studies
| Author(s)/Country | How was sleep measured? |
|---|---|
| Abdu and Dule, 2020; Ethiopia | PSQI |
| Allavena et al, 2016; France | PSQI |
| Azimi et al, 2020; USA | PSQI; Polysomnography; Visual sleep stage scoring |
| Babson et al, 2013; USA | PSQI |
| Balthazar et al, 2021; USA | Actigraphy; Sleep diary |
| Bedaso et al, 2020; Ethiopia | PSQI |
| Buchanan et al, 2018; USA | PSQI; ISI; PROMIS; Sleep hygiene scale; Sleep diary |
| Byun et al, 2016; USA | PSQI; Actigraphy; Sleep diaries |
| Campbell et al, 2019; Belgium | PSQI |
| Campbell et al, 2022; USA | PSQI; Actigraphy sleep duration and disruption; Sleep diaries |
| Chen et al, 2013; China | Actigraphy |
| Chen et al, 2021; China | PSQI; Polysomnography |
| Cody et al, 2020; USA | PSQI |
| Cruess et al, 2003; USA | PSQI |
| Crum-Cianflone et al, 2012; USA | PSQI; ESS |
| Dabaghzadeh et al, 2013; Iran | PSQI |
| Dalmida et al, 2015; USA | PSQI; ESS |
| Daubert et al, 2022; USA | PSQI |
| Ding et al, 2018; China | Jenkins Sleep Scale |
| Downing et al, 2016; USA | PSQI |
| Faraut et al, 2018; France | PSQI; Actigraphy; ESS; Obstructive sleep apnea |
| Fekete et al, 2014; USA | PSQI |
| Fekete et al, 2018; USA | PSQI |
| Gamaldo et al, 2013; USA | PSQI; ISI; ESS; Polysomnography; Actigraphy |
| Gutierrez et al, 2019; USA | PSQI; Single question: ‘Do you consider that you have a sleep problem?’; Insomnia symptoms questionnaire |
| Hand et al, 2006; USA | PSQI; ESS |
| Hixon et al, 2020; USA | PSQI; Actigraphy |
| Huang et al, 2017; China | PSQI |
| Huang et al, 2021; USA | General Sleep Disturbance Scale |
| Junqueira et al, 2008; Brazil | PSQI |
| Kunisaki et al, 2021; UK | PROMIS for sleep disturbance and sleep-related impairment; ISI; Oximetry; International Restless Legs Syndrome Study |
| Lee et al, 2012; France | PSQI; Sleep diaries; Actigraphy |
| Low et al, 2011; USA | ISI |
| Mahboobi et al, 2020; Iran | PSQI |
| Mahmood et al, 2018; USA | PSQI; SATED (Satisfaction, Alerness, Timing, Efficacy, Duration) |
| McIntosh et al, 2019; USA | PSQI |
| Mengistu et al, 2021; Ethiopia | PSQI |
| Milinkovic et al, 2020; UK | PSQI; ESS; Functional outcome of sleep questionnaire |
| Najafi et al, 2021; Iran | PSQI |
| Ning et al, 2020; China | PSQI |
| Norman et al, 1992; USA | PSQI; Polysomnography |
| Oshinaike et al, 2014; Nigeria | PSQI |
| Phillips et al, 2005; USA | PSQI |
| Phillips et al, 2006; USA | PSQI |
| Pujasari et al, 2021; Indonesia | ISI |
| Robbins et al, 2004; USA | PSQI; ESS |
| Rodríguez Estrada et al, 2018; Mexico | PSQI; ESS; Athens Insomnia Scale |
| Rogers et al, 2021; USA | PSQI; ISI |
| Rubinstein and Selwyn, 1998; USA | PSQI |
| Salahuddin et al, 2009; USA | PSQI; ESS |
| Santos et al, 2018; Brazil | PSQI |
| Seay et al, 2013; USA | PSQI |
| Shi et al, 2020; China | PSQI |
| Sun-Suslow et al, 2022; USA | Actigraphy; Single question about sleep |
| Taibi et al, 2013; USA | Actigraphy; Sleep diaries |
| Venkataraman et al, 2021; USA | PSQI |
| Vosvick et al, 2004; USA | Sleep items from Medical Outcome Study (MOS) |
| Wang et al, 2021; China | PSQI |
| Webel et al, 2013; USA | PROMIS; Actigraphy |
| Wibbeler et al, 2012; Germany | PSQI; ESS |
ESS=Epworth Sleepiness Scale
ISI=Insomnia Severity Index
PROMIS=Patient Reported Outcome Measurement Information System
PSQI=Pittsburgh Sleep Quality Index
Study characteristics
Publication dates ranged from 1992 to 2021, although interestingly one third of the articles were published in 2020 and 2021 (n=17). Over half the studies were conducted in the USA (n=35), and the majority were cross-sectional in design (n=48). Across all studies there were 25 901 participants, of whom 21 558 were people living with HIV. Sixteen studies had control groups of individuals who were not living with HIV, with a total of 4343 participants. Providing meaningful data on demographics is difficult due to lack of consistency in recording and reporting across studies. In terms of gender, 17 773 participants were recorded as male, 6520 were female and 58 were transgender. The gender of 1550 participants was not specified, in that studies would say that ‘85% of the sample were male’ but then did not explicitly state what proportion of the rest of the sample were female, trans or non-binary. The authors did not wish to make any assumptions, and therefore, unless gender was explicitly stated, we coded it as ‘not specified’. Furthermore, no attempt to summarise the race or ethnicity of participants included in the sample was made, as again there were significant inconsistencies and gaps in how these figures were reported. Race or ethnicity was not explicitly reported for 19 845 participants, which is 76.6% of the whole review sample. Furthermore, the descriptive labels used at times in studies were White-centric. For example, 705 participants had their race or ethnicity simply coded as ‘other’.
Range of methods
The review highlighted that there was a range of different methods being used to assess sleep within the reviewed studies (n=18), with just under half the studies (n=25) using more than one method to assess sleep. The most common methods for assessing sleep were the Pittsburgh Sleep Quality Index (PSQI) (n=48), actigraphy (n=11), Epworth Sleepiness Scale (ESS) (n=10), Insomnia Severity Index (ISI)(n=5), sleep diaries (n=6) and polysomnography (n=4). There was limited information provided within the studies as to why researchers had chosen to assess sleep using the particular approaches they had.
Table 2 provides an overview of the main sleep screening methods.
Table 2. Overview of different screening methods for sleep
| Name of measure | Type | Brief description |
|---|---|---|
| Pittsburgh Sleep Index (PSQI) (Buysse et al, 1989 | Self-report questionnaire | A 19-item measure covering 7 components of sleep: sleep quality, latency, duration, efficiency, disturbance, use of sleep medication and daytime disfunction.Each of the 7 components are scored 0–3, from which a total composite score was then derived. A score of 5 or over indicates a ‘poor’ sleeper.The PSQI is intended to be a screening tool, rather than a diagnostic measure. As such, it asks questions about a range of night-time symptoms related to different sleep problems such as obstructive sleep apnoea, insomnia, restless legs. It is possible for two people to screen as ‘poor’ sleepers, but for entirely different reasons: one might have insomnia and another nightmare disorder. |
| Epworth Sleepiness Scale (ESS) (Johns, 1991) | Self-report questionnaire | An 8-item measure of daytime sleepiness that does not ask about sleep directly. It is not specific to any sleep condition, although is often used as part of screening for obstructive sleep apnoea. Respondents rate the likelihood they would ‘doze off’ when engaging in various daily activities.Each item is scored 0–3, and a total score out of 24 is reported. Scores below 10 are considered normal; the higher the score, the more severe daytime sleepiness. |
| Insomnia Severity Index (ISI) (Morin, 1993) | Self-report questionnaire | A 7-item insomnia-specific measure. It covers the severity of insomnia symptoms, sleep satisfaction, impact of daily functioning, how noticeable this is to others, and the level of distress it causes.A total score is computed, which categorises a respondent's insomnia as either: non-clinical, sub-clinical, moderate or severe. |
| Sleep diaries | Self-report daily record | A sleep diary can be given to individuals to keep a daily record of their sleep and other factors that may be of interest. Typically, a respondent will record what time they go to bed, how long it takes them to get to sleep, the number of times they wake after sleep onset (WASO), what time they wake in the morning, and the time they get out of bed. It may include information such as daytime naps, record of medications, as well as amount of alcohol and caffeine consumed. This information can be used to gain a picture of someone's sleep patterns and behaviours and work out things such as average sleep. |
| Actigraphy | Objective physiological measure | Actigraphy is a method of monitoring, recording, and analysing a person's sleep–wake cycles. This is usually done over a period of a few days or a week to get a reliable picture of an individual's activity and sleeping patterns. Actigraphy monitoring is typically done using an actiwatch (worn like a regular timepiece), which contains an accelerometer that detects when the individual is moving and not moving. |
| Oximeter | Objective physiological measure | Overnight oximetry measures an individual's oxygen saturation throughout the course of their sleep. It is usually a watch-type device with a finger probe and the individual needs to turn it on and off at the start/end of their sleep. The most common reason for doing overnight oximetry would be suspected obstructive sleep apnoea. |
| Polysomnography | Objective physiological measure | The ‘gold standard’ of diagnostic sleep assessment is polysomnography; a method of recording multiple physiological variables overnight, including oxygen saturation, heart rate, brain activity (such as the architecture of sleep stages), as well as eye and muscle movements during sleep. Sometimes it is combined with video recording so it can be assessed whether these variables co-occur with parasomnia activity (eg, sleep talking). Polysomnography can therefore be used to diagnose a range of sleep disorders. |
Self-reported measures
Within the review 12 different self-reported measures for assessing sleep were used. The most common tool being used was the PSQI (n=48), the rationale being that the PSQI was identified as being a validated tool for assessing sleep. The ESS was also used (n=10), along with sleep diaries (n=6), although there was no consistent approach mentioned regarding how the sleep was recorded within the diaries. The ISI (n=5) was also used. As the self-reported sleep measures help to identify deficits with regard to different aspects of sleep (insomnia, sleep duration, sleep quality) there was a lack of consistency as to what aspects of sleep were being measured and why.
Objective measures
There were three different objective, physiological measurements of sleep used across the studies included in the review: actigraphy (n=11), polysomnography (n=4) and oximetry (n=1). In the majority of the studies using actigraphy (n=9/11), it was used in combination with other subjective measurements of sleep, such as sleep diaries (n=6) or a self-report questionnaire (n=7). This is good practice as both objective and subjective data on sleep and its impact are collected. Polysomnography was used in studies that were interested in more in-depth investigation of the physiology of people's sleep and the impact this was having.
Polysomnography requires access to specialist equipment and skills, so it is unsurprising that it was not used more frequently. Oximetry was only used in one study. It is commonly used when looking at obstructive sleep apnoea, a type of respiratory disorder during sleep that was outside the focus of this review, which explains why it did not appear more frequently in the 60 studies reviewed.
Discussion
This scoping review aimed to clearly identify what is known from the current literature on how sleep is measured within HIV care. The majority of the articles included in this review (n=48) gathered data using cross-sectional research designs, and over half of the studies reviewed (n=35) were undertaken in the USA. As such, there was a lot of replication in what the studies reviewed tell us about how sleep is currently being measured. Therefore it is important that future research into this aspect of care moves the current knowledge base forward, rather than seeking to replicate what is already known.
The homogeneity in results may be due to a number of factors. First, it could reflect the fact that the majority of studies were cross-sectional in design, and therefore a questionnaire measure was the most suitable and/or easiest to use. Second, it may be that most of the studies included in the review took a more exploratory stance about whether sleep is an important factor for wellbeing in people living with HIV. Using a screening measure that taps into different aspects or symptoms of poor sleep may reflect that the research is not at the point of investigating which specific sleep disorders or problems are key in HIV care. Several studies aimed to look at prevalence of sleep problems or a general sense of ‘sleep quality’ in HIV. What we can ascertain from clinical practice is that sleep quality is an issue that people frequently present with and therefore a design to find approaches to improving this not only a research priority, but also a clinical priority.
A final possible reason that the PSQI was used most frequently is that researchers tend to use measures that other studies have used because there is more data on the validity and reliability of the measure; the results are also more directly comparable with previous research. However, this in turn means that researchers continue to pick a given measure for these reasons, rather than it necessarily being the best measure to use. Indeed, some studies suggest that there are methodological issues with using the PSQI to accurately detect the presence of sleep issues and any change in sleep that may occur (Faulkner and Sidey-Gibbons, 2019). Furthermore, the lead author of the PSQI has since gone on to develop a new sleep measure, the PROMIS (Buysse et al, 2010, used in n=3 studies in this review), in light of the fact that the individual items of the PSQI had not been psychometrically evaluated, and the use of a total PSQI is not consistent with factor analysis (Cole et al, 2006).
Although the PSQI was by far the most favoured method of measuring sleep, a variety of different approaches was used across the studies (n=18). This means that there were differences with regard to which aspects of sleep were being explored, but not much information was provided on why these aspects were being investigated, and why researchers had picked specific methods to do this. It is important that future research design gives careful thought about which aspect of sleep is of interest and how best it can be measured to ensure that the insights gathered as a result of the research can be used to enhance patient care.
Another finding to consider is the context in which research was undertaken when interpreting the relevance of how sleep is being measured within HIV care settings. We found no articles within the review that explored sleep data collected as part of routine care; as far as we could determine, all sleep measures and data were collected for a finite time period specifically for the purpose of the research. It was not evident from the articles reviewed whether this then became a standard of care based on the research findings.
Across all the studies, 80% of the participants living with HIV were male. This is not representative of global statistics, because over half of the people living with HIV worldwide are cis-women. Moreover, trans people made up only 0.27% of participants living with HIV. Given global prevalence estimates, this is a significant under-representation of the trans community in the research. Similarly, information on race and ethnicity was not recorded for 76% of participants. Lack of representation and diversity in research limits the generalisability of findings regarding sleep, and how best to measure it, in people living with HIV.
Strength and limitations of the review
A key strength of a scoping review is that it provides a thorough overview of an area of research (Arksey and O'Malley, 2005). Unlike systematic and meta-analysis reviews, criteria for inclusion and exclusion are based on relevance not quality. Therefore, the studies reviewed varied considerably in sample size and the focus of investigation. As such, this is a descriptive account of how sleep is measured in HIV care and not a critical analysis of the current research.
Our review has several strengths. We used a comprehensive search strategy across multiple databases, and the process of including and extracting data was undertaken by two researchers to enhance the credibility of the scoping review (Levac et al, 2010). In addition, the research team consisted of researchers with expertise in literature searching, HIV, and sleep.
However, despite our inclusive search strategy, it is possible that our approach was limited by factors such as the search terms used, and the choice of database being limited by institutional access. To mitigate this, we hand-searched reference lists for missing articles and requested these separately where possible. An additional limitation was the decision to include only empirical studies; however books and grey literature were included at the initial search phase, but a title and abstract scan indicated that these sources did not contain relevant information. We excluded research undertaken as part of HIV medication clinical research trials because sleep was not the focus of the research. We likewise excluded papers that focused exclusively on obstructive sleep apnoea: we made the decision that because this was a respiratory condition it was a confounding variable. We also did not look at the reported outcomes of the studies reviewed because this was not the aim of our review, and we wanted to keep a tight focus on exploring measurement.
Implications for future research
An important recommendation of this review is that future research into the sleep of people living with HIV should be more specific about which aspect of sleep is being investigated and why, so methods and measurements are selected accordingly; explicitly explaining the rationale behind this.
Research should also look to be more inclusive and diverse when it comes to recruiting participants, so that their findings are more generalisable to the larger populations of people living with HIV. Moreover, the gap between research and clinical practice needs to be bridged so that findings are being translated into better care.
Implications for clinical practice
Our results may help health professionals to consider the multivariant nature of measuring sleep to effectively enquire about sleep within HIV care. Those working in clinical practice must use measures as they are intended and with due clinical interpretation to avoid a bias towards assuming reported poor sleep quality is synonymous with insomnia or poor sleep hygiene. The way in which the PSQI data were reported in studies within the review gave no indication that researchers were considering which items participants had endorsed, meaning they were not discriminating between the different types of problems and symptoms that might be causing poor sleep.
Clinicians need to be more aware of the different types of sleep difficulties and disorders there are, consider the aspect of sleep that they are concerned about and then choose suitable tools to explore this. That is not to say that screening tools such as the PSQI do not have utility. Sometimes service users and clinicians are unsure what is causing poor sleep, so using screening tools such as the PSQI and/or sleep diaries can be a useful starting point. The key thing to remember is that they are just that, a starting point, and the next steps in providing care must be grounded in the clinical information gained.
KEY POINTS
- The HIV care landscape has changed significantly over the past 30 years, with quality-of-life issues increasingly significant in the consultation room
- It has been identified that sleep, and finding ways to enhance sleep, is important when exploring how to improve outcomes for people living with HIV
- Sleep is a multifactorial construct, so we need to be thoughtful about what aspect of sleep we are interested in and how best to measure it to obtain meaningful data and ultimately improve sleep health
- There needs to be more research that explores and provides meaningful recommendations for clinical practice
CPD reflective questions
- Consider the impact of poor sleep, and how this could impact on an individual living with HIV. You may want to consider factors such as how it could affect someone's mood, cognitive functioning and ability to engage in daily activities. How might this influence adherence to medications, or attendance in clinic?
- Do you routinely ask about sleep in clinical appointments? What could this look like? Are there any questions or brief measures you might use to open up a conversation?