

Sarcomas develop throughout the body in bones and connective tissues; they are a group of rare, often aggressive cancers (Sarcoma UK, 2024). Bone sarcoma is extremely rare and makes up 0.2% of all cancers in the UK (Schaser et al, 2009; Sarcoma UK, 2024) while sarcoma of the spine is even rarer, with approximately 100 new diagnoses per year, based on the number of patients presenting to the four spinal centres in the UK. On average 500 patients each year are diagnosed with a bone sarcoma. The four most common types are chondrosarcoma, osteosarcoma, Ewing's sarcoma and chordoma (Sarcoma UK, 2024). According to the Bone Cancer Research Trust (BCRT) chordoma is the most common sarcoma to arise in the spine and affects mostly adults in their 40s and 50s (BCRT, 2024). Symptoms of bone sarcoma include a mass or swelling, pain particularly at night, restricted movement in a joint or loss of function in a limb (BCRT, 2024). An X-ray can be sufficient in showing abnormalities suggestive of bone sarcoma, which would warrant referral to a specialist sarcoma service. Diagnosis requires clinical examination, further imaging, and a biopsy (National Institute for Health and Care Excellence (NICE), 2020).
The Oxford Spine Sarcoma Service is a dedicated spinal surgery service and is one of four nationally commissioned centres for the treatment of primary bone and soft tissue sarcomas of the spine, serving a population of around 10 million (Office for National Statistics, 2024). Delays in referrals and confirmation of a diagnosis continue to lead to significantly poorer patient outcomes, causing additional emotional distress (NICE, 2020). Due to the rarity of sarcoma, patients can understandably feel isolated with limited support and information (George and Grimer, 2012).
After a patient and public involvement (PPI) event, funding was secured for two registered nurses to be seconded as research nurse interns at the start of the project. The Oxford Spine Sarcoma service decided to facilitate a project in which patients were paired as ‘buddies’ to trial a patient-requested peer-to-peer support programme within the service.
It is acknowledged that charities such as Macmillan Cancer Support facilitate peer-to-peer support for people diagnosed with more common cancers, such as breast cancer (Macmillan Cancer Support, 2024). This is echoed in the published literature, where the effectiveness of peer-to-peer systems in a variety of healthcare settings has been explored (Weaver et al, 2020). However, there is limited literature on, or charity-funded support for, rare cancers in relation to peer-to-peer support systems. Benefits of peer-to-peer support in oncology care have been documented in the literature (Jansen et al, 2023; Tan et al, 2023). A recent systematic review, which included 29 papers, identified that peer support led to an increase in psychological empowerment and was associated with further patient-reported benefits (Ziegler et al, 2022). The review highlighted a need for further studies with long-term follow-up and larger sample sizes. Another recent systematic review by Kiemen et al (2023) identified a need for more randomised controlled trials with high methodological standards to evaluate the effectiveness of peer support.
The aim of the project was to determine the acceptability and feasibility of a peer-to-peer support project among spine sarcoma patients. To achieve this, the objectives were:
- To explore a peer-to-peer support system within the sarcoma service
- To develop a voluntary peer support group
- To build a network of ‘buddies’
- To measure the outcomes.
Methods
The idea of creating the peer-to-peer support system came from a PPI event that was organised by the Oxford Spine Sarcoma Service. For this PPI event, service users of the spine sarcoma pathway were invited to their local Maggie's Centre, a charity providing free cancer support (Maggie's, 2022), to explore the unmet needs of patients and their family members. The PPI event identified the need to develop a team who have lived experience and first-hand encounters with the spine sarcoma service to support new patients coming into the pathway. A peer-to-peer patient support system called the ‘Buddy Project’ was planned.
Following the event, a clinical trials and research governance application (CTRG) was completed for local ethical approval. The project was approved by the Trust research and development team as a service evaluation with the aim of improving the service by providing a peer-to-peer support system.
The ‘buddies’ for the project were self-identified from previous service users and invited into the peer-to-peer support programme through the voluntary services team at Oxford University Hospitals NHS Foundation Trust. In the context of the project a buddy is someone who has been diagnosed with or cared for a person with primary bone or soft tissue sarcoma of the spine and is happy to share their experience with others seeking support.
Sixteen people initially expressed their interest to be buddies; however, only four of the participants were able to complete the mandatory checks and training within the time constraints of the funded internship (Figure 1). The four participants were then matched with each other at random to reduce the risk of bias. The patient information sheet and posters regarding the ‘Buddy Project’ were sent by post to all interested participants. Written and verbal informed consent was obtained from all participants, and their decisions to participate documented in the electronic patient record (EPR).
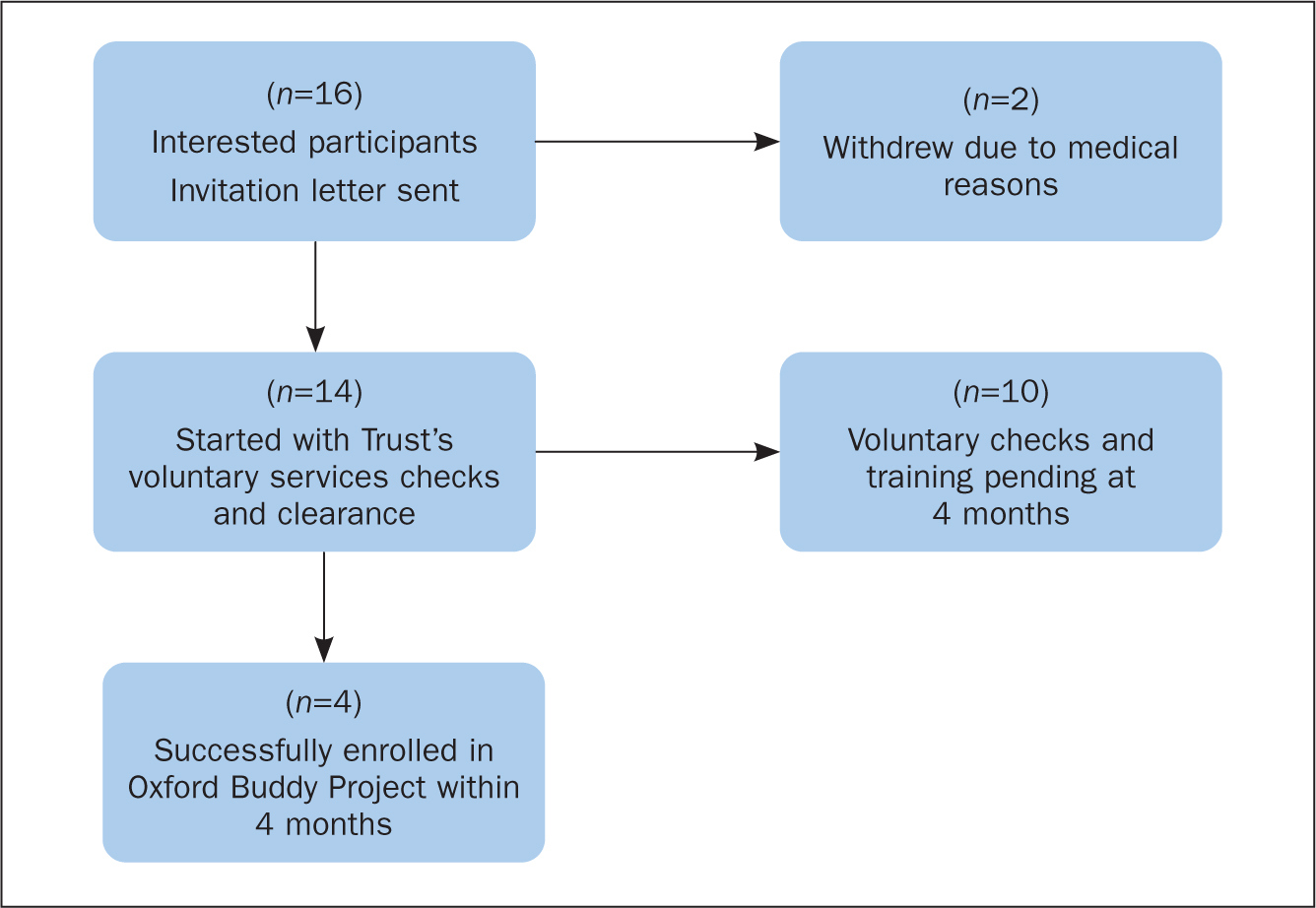
Induction into the peer-to-peer support system required some preliminary checking. ‘Buddies’ were selected and trained through the voluntary services department and its standardised Trust-approved process. Table 1 shows the mandatory checks and training that the buddies needed to complete to participate. The feasibility project was funded for a period of 6 months; due to time pressures, the aim was for voluntary services checks and training to be completed within the initial 4 months. Unfortunately, 10 participants were delayed in processing through the voluntary services clearance checks and training within the planned timeline. Therefore, the sample size was considerably reduced. However, interested participants were followed up to be included in the next available cohort of Oxford Spine Sarcoma Buddies.
Table 1. Mandatory checks and training for ‘buddies’ (as required by voluntary services)
| Mandatory checks | Mandatory training |
|---|---|
|
|
Due to social distancing restrictions during COVID-19 the meetings had to be organised through online platforms and telephone conversations. Microsoft Teams was used for online meet-up sessions. None of the buddies dropped out of the study and all interacted well via Microsoft Teams. However, provisions were in place such as a nurse intern being present online but not actually in the meetings via the use of Microsoft Teams breakout rooms. Buddies could then contact the nurse if they needed to raise any concerns.
A mixed-methods data collection approach was used with the aim of exploring the experiences of patients and their relatives to identify the effectiveness of the intervention of introducing a buddy and the potential need for future support systems. A mixed-methods approach was chosen to measure patients' perspective on peer-to-peer support subjectively as well as through a standardised satisfaction questionnaire, enabling the data sets from both approaches to complement each other (Regnault et al, 2017).
Quantitative data
Anonymised electronic questionnaires were sent out prior to the buddies being introduced to gather data on their satisfaction with the service. Data were collected using the Client Satisfaction Questionnaire (CSQ-8) (Attkisson and Greenfield, 1996). The CSQ-8 is a standardised tool used to measure satisfaction across various health and human services (O'Regan and Ryan, 2009). The CSQ-8 questionnaire consists of eight questions, each with response options from 1 to 4. A minimum overall score of 8 indicates low satisfaction, a maximum score of 32 indicates high satisfaction with the service (Attkisson and Greenfield, 1996).
Following the buddies being introduced and meeting up several times, a second set of CSQ-8 questionnaires were sent to assess post-intervention patient satisfaction.
Qualitative data
Qualitative data were collected through semi-structured interviews. The interview questions were open-ended questions, sent as Microsoft Forms to the participants to fill in and later followed up by the research nurse interns via phone call. The communication was recorded, and verbatim transcription was used. Once transcribed the audio data were deleted. The interviews lasted 10-15 minutes, scheduled according to participants' convenience. The calls were made using the Trust telephone to ensure confidentiality. The transcription was read independently by ST and JC and common themes identified through pragmatic thematic analysis (Green and Thorogood, 2018).
The participants were invited for an induction session. During this session detailed descriptions and explanations of the peer support system were given. Buddies had the opportunity to ask questions, and expectations from the buddies were also shared. The session included presentations on confidentiality, data protection, safeguarding, and escalation pathways for concerns that a buddy or patient may have. Following the induction, the buddies were randomly paired to assess the feasibility and acceptability of the support system. The meetings took place over MS Teams video calls, with one of the research nurse interns being present online while the buddies meet in a separate virtual room.
Findings
The demographic details in Table 2 represent the total number of buddies who were successfully recruited for the initial peer-to-peer support group. During the period September 2021 to March 2022, four participants cleared all preliminary checks sent by the voluntary services department.
Table 2. Demographic details of participants
| Participant | Gender | Age | Diagnosis |
|---|---|---|---|
| 1 | Female | 34 | Giant cell tumour |
| 2 | Female | 40 | Chordoma |
| 3 | Female | 52 | Giant cell tumour |
| 4 | Male | 64 | Chondrosarcoma |
The mean age of the group was 47.5 years, with participants ages ranging from 34 years to 64 years. The mean CSQ-8 score before introducing the buddy project was 26. Three (75%) of the participants agreed that the quality of service received from the spine sarcoma service was ‘good’, one (25%) responded that the service was ‘excellent’. All four responded that all or most of their needs were met through the service.
After being paired with a buddy, the mean CSQ-8 score was 26.75, with a range between 24 and 32. Two (50%) responded that they would recommend the service to someone in a similar situation and two (50%), said they would recommend the service.
‘Before’ interviews
The semi-structured interviews performed before introduction of the buddies brought out the following themes.
Concerns
Participants expressed their concern in sharing their experiences with another person new to the service. The buddies voiced their opinion that the task of giving a realistic view to the support seeker was essential, but at the same time they would have to ensure that they were not overwhelming the person with facts about what was going to happen. One of the participants commented that when sharing experiences:
‘One thing you've got to be careful about is that everybody's got their own experience on what they went through, and you don't necessary want to scare anybody, or make them even more sort of nervous.’
Participant 3
Experience in supporting or volunteering
The buddies were confident to support another person in their sarcoma journey and were willing to share their experience with someone new to the spine sarcoma service. Although many of the buddies were not professionally trained to be support workers, all of them said they wanted to help by sharing from their own experiences.
Expectations about the buddy project
The buddies were looking forward to starting the project as they agreed the support system was a means to help and support new patients by sharing their knowledge and personal experience.
‘To be in this project, it was just to give them hope and for them not to feel [as] lonely as I felt.’
Participant 1
‘After’ interviews
After the buddies were paired and had interacted with each other through MS Teams a second interview was set up to assess the acceptability and feasibility of the support system.
Benefits of the buddy system
The buddy project system was an opportunity to reassure another person with spine sarcoma that:
‘… they are not alone especially when you are going through it, because you feel alone and not understood.’
Participant 1
An open and honest conversation shared from lived experiences enabled participants to empathise on a deeper level. They felt they were:
‘… supported and understood, unlike talking to a friend who is empathetic but doesn't understand it as they didn't go through it.’
Participant 1
The buddies unanimously agreed that they could find an enormous difference in having a buddy to support them in their journey because they could compare this experience with the time previously, where they were feeling ‘quite alone’(Participant 2) and found it ‘quite daunting’ (Participant 2) or were ‘not understood’ (Participant 1). Although being allocated a buddy after treatment and rehabilitation was not as necessary as at diagnosis, the opportunity to compare stories and identify gaps in social support was welcomed.
Introduction of buddies
The ideal time to be paired with a buddy in the spine sarcoma pathway was perceived differently by individual participants, some had mixed opinions. Three of the buddies agreed that the buddies could be introduced at time of diagnosis or soon after that as ‘they can tell you what to expect’ (Participant 3). However, one of the participants said that:
‘I can't really say, because I can't sort of think about how I felt at the time whether I would or would not have wanted to talk with someone.’
Participant 2
Spine sarcoma surgeries are unique and tailored for each patient therefore it was suggested that they should be paired during later stages of the treatment path.
Need for support
The need for support was identified, and the idea of providing support was welcomed. One of the buddies was undergoing treatment and therefore could relate their experience to that of their support buddy. They shared their experiences of various aspects of treatment and how they dealt with certain situations:
‘This works for me and that works for you.’
Participant 2 and Participant 4
Although the buddies had different diagnoses and different treatment modalities, ‘to empathise with you a lot’ (Participant 2) was highlighted as beneficial. The need for peer-to-peer support was much appreciated as this provided a chance for the buddies to speak about things that they would not have otherwise talked about with the doctors or medical staff:
‘You don't feel comfortable in telling whatever to your consultant because he is your main surgeon, you see him about big problems and that's it, you have other questions that are not so important but they are important for us.’
Participant 1
The need for peer support in particular was identified:
‘It helps to talk with someone who isn't a friend or relative, I went to social media sort of sites and groups to talk to people, to find out their experiences.’
Participant 2.
The participants emphasised the difference of sharing lived experiences:
‘When you talk to someone like a friend who is empathetic, they don't really understand it and I feel that participant 3 also felt the same, I have [a] lot of support, but I need someone who can understand what I feel.’
Participant 1
One of the participants mentioned about the difference of having a rare diagnosis such as sarcoma:
‘It's something so new that even people that went through cancer don't relate [to], because we don't go through chemo, and we don't go through other stuff that they are going through.’
Participant 1
Discussion
As previously mentioned, the literature with regard to peer-to-peer support for patients with sarcoma is scarce. A study on ‘the unmet needs of patients with sarcoma’, by Weaver et al (2020), found that support interventions are needed to help patients adjust to sarcoma and to improve their quality of life as an outpatient. Weaver et al identified several themes, two of which included a lack of information and need for a community. Sarcoma patients in the study described a need to connect with others who had gone through a similar experience. They concluded that connecting patients with sarcoma support groups might provide them with more relevant and intimate support. Our findings agree, and support the need for an ongoing peer-to-peer support system especially within a rare tumour service.
The experiences and journeys of bereaved relatives of those with a sarcoma diagnosis has also been explored, highlighting that sharing experiences is useful in gaining support and managing to cope (O'Connor et al, 2021). The literature suggests that supporting relatives of those who have received a sarcoma diagnosis also encourages and enables them to better support their loved one. Therefore, during the peer-to-peer support system intervention relatives of those with sarcoma were invited to participate in the project.
Participants voiced their frustration of feeling alone due to at times a lack of information and support. A study in Birmingham involving 107 patients, 41 of which were diagnosed with bone sarcoma, identified the need for greater awareness of sarcomas through amendments to guidelines, clearer referral pathways and more robust education strategies for health professionals (George and Grimer, 2012).
The study recognised that although patients can also contribute to their own delays in diagnosis, this is difficult to reduce as widespread public awareness would result in undue public concern and an increase in unnecessary referrals. Therefore, while promoting sarcoma awareness and ensuring clearer guidelines and pathways it would also be beneficial for support systems to be in place for patients to feel less alone (George and Grimer, 2012).
Limitations
There were several limitations of the project. One of the main constraints was the COVID-19 pandemic and the government's social distancing restrictions. The project team had hoped that buddies would be able to interact face-to-face at the Maggie's Centre in Oxford. However, buddy meetings had to instead be held online via MS Teams due to restrictions. A few participants struggled with computer literacy, which prevented them from completing the relevant checks and documentation to be a buddy. Time restraints, including the length of wait for health checks and Disclosure and Barring Service (DBS) verifications, were other limitations of the project. These verification checks were requested by the Trust voluntary services team along with an occupational health clearance, which took several weeks. This reduced the number of participants who were initially able to be paired.
The project team recognises there were limited participants and even though sarcoma is rare, with on average 5300 people being diagnosed in a year (Sarcoma UK, 2023), it can affect a wider patient demographic with regard to age than included here. Lack of time was also a limitation of the project as the funding was secured for two research nurse interns for only a 6-month period.
Conclusion
A need for support within this complex oncology cohort has been met and well received. Participants in the project felt that being allocated a buddy, especially at diagnosis, would be beneficial and increase their level of support. Based on the encouraging early findings from the first four participants, the team is continuing to roll out the buddy programme within the Oxford Spine Sarcoma Service. Further evaluation of the programme will continue and future efforts will be disseminated.
KEY POINTS
- Spine sarcoma is rare. Literature shows patients often receive delays in referrals for investigation and assessment and confirmation of diagnosis, feeling isolated
- There is limited support and dedicated patient information available nationally
- The project identified that participants felt ‘less alone’ after meeting with a buddy and the need for support was welcomed
- The time to be paired with the buddies in the spine sarcoma pathway was perceived to be different for different participants
- A peer-to-peer project with an increased number of participants would be useful in further assessing the need for support
CPD reflective questions
- How useful do you feel a peer-to-peer support system would be within your service and why?
- What feedback, if any, have you ever received from patients about peer-to-peer support?
- Within your service, what could be the potential challenges of patients being allocated a buddy?