
In the UK, around 42 000 people are diagnosed with bowel cancer each year. Associated risk factors, such as obesity and poor diet, are prevalent in the UK but patients who receive an early diagnosis (stage 1) have a more than 90% survival rate at 5 years. This drops significantly to less than 10% in those diagnosed at the latest stage (stage 4) (Cancer Research UK, 2019). With the emphasis on early detection, the Government produced a White Paper in 1997, stating the intention that by 2000 all patients assessed by a GP with a suspicion of bowel cancer should be referred to and seen by a specialist team within 14 days (Department of Health (DH), 1997). This would be vital to ensure that the NHS Cancer Plan targets of 62 days between referral and first treatment and 31 days to treatment after diagnosis could be met (DH, 2000) and led to the development of the ‘two week wait’ (2WW) clinic.
Although the primary purpose of a 2WW service is early cancer detection, further goals include the development of better partnerships between primary and secondary care and delivering a timely and consistent service (Vulliamy et al, 2016). Progress made in the development of pathways such as ‘straight to test’, ‘direct to test’ and the 2WW service has improved survival rates and seen the number of people referred by their GPs rising to over 1.7 million in 2017, compared with 500 000 in 2014 (NHS England, 2017). ‘Straight to test’ (where patients are sent directly for blood test and a flexible sigmoidoscopy) and ‘direct to test’ (where patients are sent directly for investigations, such as CT scans or colonoscopies) are alternatives to the 2WW pathway (NHS Cancer Programme, 2018). However, although these may promise a reduction in duration of diagnostic time (Flashman et al, 2004), 2WW clinics demonstrate a significantly greater diagnostic yield of bowel cancer and a reduction in the number of investigations patients undergo (Flashman et al, 2004). This is alongside a statistically significant survival rate (Bhangu et al, 2011), identifying the ‘red flag’ driven 2WW approach as both effective and valid.
Elsewhere in Europe, similar approaches are taken in the form of a standardised cancer patient pathway, which identifies ‘red flag’ symptoms and guides investigations and treatment (Probst et al, 2012). However, a study in Denmark by Jensen et al (2014) concluded that, despite the pathways, GPs suspected cancer more frequently than they made referrals, especially if the symptoms were considered vague (Jensen et al, 2014). In what may have been a partial response to these findings, the guideline from the National Institute for Health and Care Excellence (NICE) on the recognition and referral of suspected cancers was revised and updated in 2015 to include less specific symptoms of weight loss and abdominal pain—it was revised again in 2017 (NICE, 2017a). This in turn led to a rise in referrals from primary care and the need for improved service delivery.
Development of the service
Historically, the authors' acute hospital trust provided a geographically blind service whereby patients were fitted into existing consultant clinics. Due to the ad hoc allocation of appointments, patients were often not seen until day 14 on their cancer pathway. Furthermore, they were predominantly assessed by very junior medical trainees with minimal colorectal experience, resulting in variation of both assessment and test selection. This is in direct contrast to aims set out in the 1997 White Paper, and recognising this problem led to the planning and development of a new service.
Driven by the colorectal consultant nurse and the specialty lead consultant, standard operating policies were written and a pro forma-based assessment was developed to ensure consistency across the service. These were reviewed by the gastrointestinal directorate and the governance board before being submitted for Trust approval. A protocol was developed in conjunction with the radiology and endoscopy departments to ensure a structured approach to test selection and to aid business cases, ensuring that capacity could be planned to meet demand.
Referral
A standardised referral letter was generated and distributed to the primary care providers in order to garner relevant medical history prior to a clinic appointment, which was an important aspect in developing an efficient paperless approach to the service. Completed referrals are faxed by primary care to the acute trust's booking office and uploaded on to the patient's electronic hospital record. With guidelines in place, all appointments were centralised to the acute trust, which allowed a greater flexibility based on demand. A capacity of 90 clinic slots, an increase from 56, was generated on a weekly basis, with appointments available between 24-48 hours from referral, in sharp contrast to the previous waiting time of 14 days. Following receipt of the referral from primary care patients are allocated to 20-minute clinic slots by the booking office.
Nurse training
Experienced colorectal nurses were put through a rigorous in-house training programme, which included a higher education qualification in patient history, examination at the local university and training within the department. This consisted of demonstration, direct supervision and formal assessment by the colorectal consultant nurse and consultant surgeons.
The specialist nurses were progressed through a process that started with observing the consultant nurse undertaking several clinics plus pro forma and protocol teaching. Following this they performed a modified version of the usual clinic with fewer patients and 30-minute slots per patient, observed by the consultant nurse. When both the consultant nurse and specialist nurse felt confident with the clinics, a colorectal consultant assessed the nurse. On successful completion of the assessment, the specialist nurse was permitted to undertake the clinic (in its reduced format) with a qualified member of staff rostered nearby for support and advice. Finally, once the specialist nurses felt confident in these clinics (around 2 months), they were formally assessed by a second consultant and were then permitted to conduct full independent clinics.
All specialist nurses conducting independent 2WW clinics are required to have passed the Ionising Radiation (Medical Exposure) Regulations (IR(ME)R) training and to practise within the confines of the clinical guideline agreed through the hospital's governance process, which sets out which investigations the specialist nurse is permitted to request.
In order to be qualified in autonomous sign-off for test results, the specialist nurses undergo training by the consultant nurse and specialty lead consultant. Training consists of two independent face-to-face assessments and the provision of evidence in the form of log books.
Telephone clinics
Initially, all patients were assessed on a face to face, however restrictions on available clinic space meant that the increased capacity was hindered not by staffing, but by limited resources. In a largely rural community patients referred to the bowel 2WW service were potentially travelling substantial distances with significant loss to personal time, not to mention incurred parking expenses. These two issues highlighted a need to change the team's approach to service delivery and, after extensive discussions, telephone assessments were considered a suitable option for patients who met specific criteria identified within the assessment guidelines.
Protocols were expanded to allow for telephone consultations and patients were excluded from this based on symptoms deemed to require a physical examination, such as a rectal or abdominal mass (Mealie and Manthey, 2019) or age, with any individual aged over 80 years excluded due to the increased likelihood of comorbidities and impact on general health (Divo et al, 2014).
All remaining patients were deemed suitable for assessment over the telephone. However, due to variation in the population's health—it is usually assumed younger people have fewer comorbidities, but this is not always the case—the team are able to request a change in appointment if there are any concerns during the telephone assessment or anything is identified on the GP referral letter prior to assessment. As the waiting times are consistently low this does not cause more than a few days' delay.
In 2018, the team was able to secure exclusive rights to permanent clinic facilities, which has not only prevented a bias towards providing telephone clinics, but has also allowed the running of parallel clinics (one telephone, one face to face) when referrals are at a peak.
The telephone side is arguably more difficult in terms of clinical decision-making because clinicians are not afforded the benefit of an ‘end-of-bed’ assessment and, as previously stated, even young people can have multiple comorbidities (Divo et al, 2014). Assessors are heavily reliant on obtaining accurate and truthful responses from patients, and decisions have been made to send individuals for investigations who might not have been considered had they been seen face to face. It goes without saying that two 60-year-old patients can have vastly different health outcomes (Piccirillo et al, 2008). For this reason, telephone assessments are undertaken only by those who have significant experience in the face-to-face format and are therefore more practised at picking up on verbal cues (Car et al, 2004).
Assessment and tests
The use of a pro forma has been shown to reduce the occurrence of ‘missing’ clinical information, by acting as a prompt for those undertaking the assessment (Kentley et al, 2016). All bowel 2WW appointments consist of a paperless pro-forma assessment, which allows space for free text to expand on a patient's individual symptoms and medical history. Any patient assessed in a face-to-face appointment will also undergo an abdominal and rectal exam, with their consent. Telephone assessments rely on this having been carried out by the referring GP and, in instances where this has not been done, they are requested to undergo this prior to investigation, either at their surgery or by coming to the hospital and having one of the team carry this out. The rectal exam and routine blood screening for haemoglobin, ferritin and estimated glomerular filtration rate (eGFR) are marked mandatory on the referral form and are in line with guidance from NICE (2017a).
At the end of the assessment the protocol is used to determine the most appropriate test for the patient and the procedure is explained in full prior to booking. There are instances in which patients are not happy to undergo the more invasive investigations, and the clinician may need to deviate from the protocol in order to complete bowel investigations, but this can often be circumvented by providing thorough patient education (Fowler et al, 2011).
More recent service improvements have seen the specialist team now booking some tests (endoscopy) during the initial assessment. The waiting period between assessment and endoscopic investigation has now been reduced to 5 days, ensuring efficiency of the patient's journey through the suspected cancer pathway and improving the trust's ability to meet the national cancer targets.
All investigations are booked under the umbrella of bowel 2WW rather than the named clinician and are reported into a centralised location. All results (an average of 480 per month) are checked within 4 days of reporting and admin is completed solely by the nursing team. Decisions are made by the nursing team regarding the requirement for additional investigation, for example, where the result is of poor quality, whether patients should be referred to the lower gastrointestinal (GI) multidisciplinary team (MDT) or another service for incidental findings or whether they can be discharged back to the care of their GP (Table 1). Where non-bowel cancers are identified, the results are reported directly to the colorectal consultant nurse for urgent referral to the appropriate specialty.
|
|
Occasionally, patients have been referred to the service who either do not meet the referral criteria or who have recently been investigated and have had bowel cancer excluded as a cause for their symptoms. In these cases, a routine appointment may be made to see a consultant to discuss the management of ongoing symptoms or they may be discharged back to their GP where appropriate.
Barriers and challenges
The team has faced a number of challenges. One team member was due to move out of county, meaning the loss of a fully trained service provider. However, the implementation of telephone clinics has meant that they can continue to work for the team, albeit very remotely, allowing the service to continue unaffected. The training programme is intensive, which means that, although team members are well trained and supported throughout their supervisory period, it is a slow process and so with an exponentially increasing number of referrals, the burden of service provision lies with those already fully trained. One of the main areas of difficulty is securing ongoing funding from the acute trust for a rolling employment programme, which would ensure the security of the service and future-proof the workforce.
Although predominantly nurse led and delivered, the service is still reliant on occasional (but invaluable) support from medical colleagues (for example, during periods of sickness or annual leave). Although junior medical colleagues are a welcome asset for the service, the transient nature of their training results in a continual need to provide training in the protocol and pro forma before they move on, and the next new doctor requires further training. However, with ongoing recruitment the aim would be to deliver a purely nurse-led service. It is interesting to note, based on a local audit of investigations booked over a 2-year period that the nursing cohort consistently adhered to local guidance and protocols for booking to test. This finding is not limited to the trust in question; in 2005, McDonald et al concluded that nurses equated adherence to guidelines with professionalism. If their hypothesis is accepted, then patients could stand to benefit from the safety culture offered by a solely nurse-delivered service (McDonald et al, 2005).
The Health and Social Care Act 2012 brought about the establishment of Health Education England, whose goal was to identify and meet patient needs by establishing a workforce that ensured the right people with the right skills were delivering safe and effective care. There is a clinical and financial need within the NHS to provide a workforce sufficient in numbers not only to meet service demands but also to allow the development of other health professionals, if trusts are to achieve the aims of the Five Year Forward View (NHS England, 2014) This is all with an aim of creating a sustainable, well-equipped specialist cohort who are in the correct place to offer appropriate care (Addicott et al, 2015). The role at a local level is to address immediate gaps in service provision, such as the challenges faced by the colorectal team in the provision of a 2WW service.
Key workforce drivers, as identified by The King's Fund (Addicott et al, 2015), include investment in the training of health professionals with a view to producing an adaptable workforce responsive to the long-term needs of the service user. Junior doctors, who are often used to support services such as the bowel 2WW, are essentially a transient workforce, so the time (and ultimately, money) spent training them to carry out the role would be put to better use in developing a nursing cohort that is fit for purpose and able to provide longevity, which their junior medical colleagues cannot.
NHS England's business plan Putting Patients First (NHS England, 2013a), an expansion to Everyone Counts: Planning for Patients (NHS England, 2013b), identifies 11 areas of care in which improvements could be delivered; the primary goal was to increase patient satisfaction and improve workforce morale, both of which are key performance indicators of high-quality care provision (Prakash, 2010). Although written in 2013, the ideology and academic evidence behind the drive remains intact.
Patient satisfaction and outcomes
At the beginning of 2015 a prospective, non-randomised comparative cohort study was undertaken to determine patient satisfaction with the 2WW service (Cock and Kent, 2017). This had a twofold aim: to explore overall satisfaction with the service and to determine whether this was affected by its delivery through medical or nursing health professionals. All patients due appointments within a 3-month period were invited to participate and were then allocated clinic slots by the booking team (who were blinded to the clinician) based on availability. A validated ten-point questionnaire was used to measure patient satisfaction, using both positively and negatively worded questions; and a free-text box was provided for additional comments. Results showed that although there was a generally positive response (96.9% of patients either strongly agreed or agreed that they were very satisfied with the care they received), significantly more patients expressed strongly-agreed responses in the nurse-led cohort, which was further substantiated after analysis of the free text.
Audits are ongoing to investigate patient satisfaction with the telephone service, which to date have highlighted a positive patient experience. From a secondary care perspective, a telephone assessment service is resource light and additional clinics can be added at short notice to comply with demand, thereby ensuring greater flexibility. From the clinical side, an annual audit of key performance indicators is carried out to determine the number of colorectal and other cancers that are identified, in order to compare local and national data.
An audit was carried out on retrospective data collected between January and June 2017. In all, 1603 appointments were allocated during that period (excluding patients who did not attend) and, of these, 59% were conducted over the telephone; 5% of patients were referred directly to a colorectal consultant on a 2WW basis as a result of findings at initial assessment. Of the patients referred to test, two-thirds were sent for endoscopy while the remaining third underwent radiological investigation; 5% of the patient population did not attend their booked investigations.
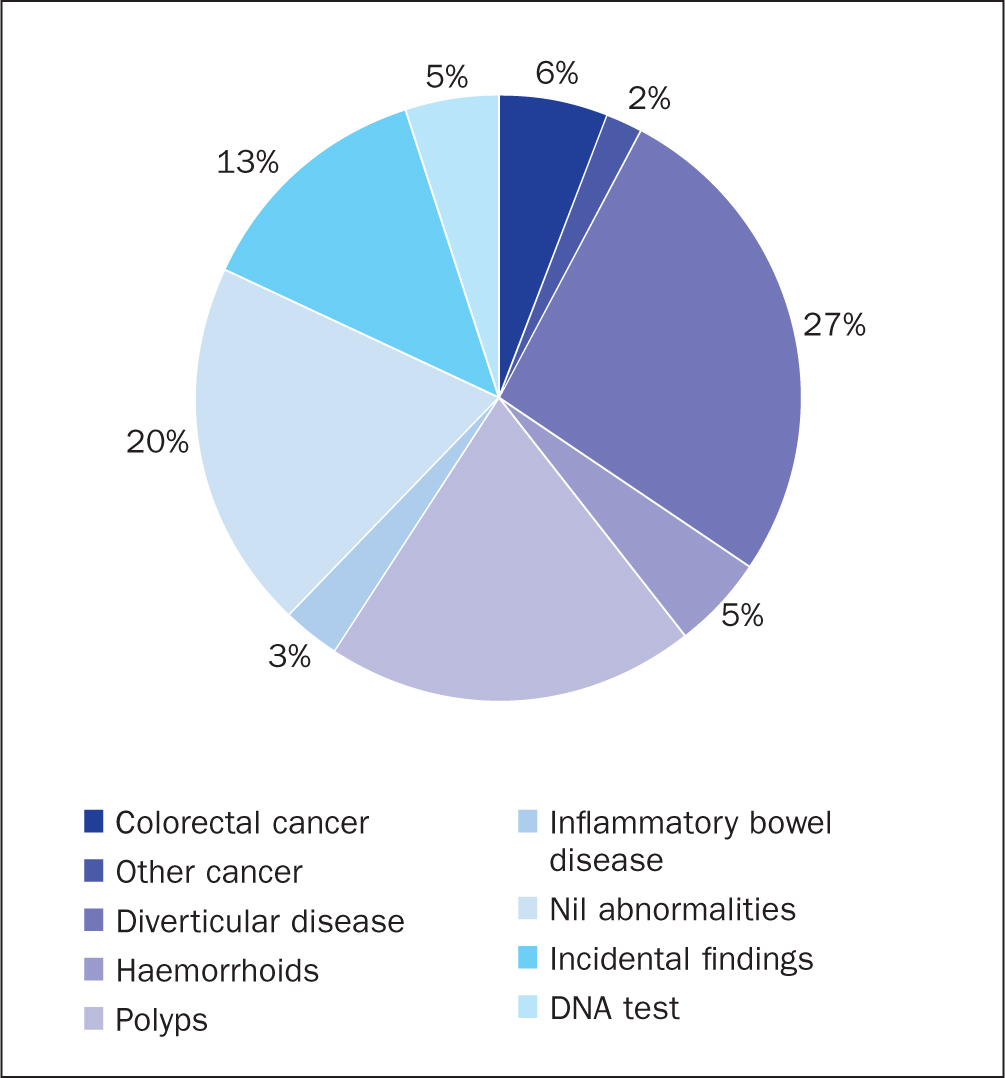
Within this 6-month period, colorectal cancer was identified in 5.8% of patients while incidental findings of other cancers were 1.9%. Non-sinister bowel pathology such as colorectal polyps (19.9%), diverticular disease (27%) and inflammatory bowel disease (3%) were also identified; in 19.7% of patients no abnormalities at all who were found (Figure 1).
On the basis of these reports, 73% of patients were discharged back to the care of their GPs, 9.3% were booked for polyp surveillance after a set period of time, 6.3% were referred to the lower GI MDT and 4% were booked to see a consultant on a routine basis.
Further developments
In June 2015, NICE suspected cancer referral guidelines were broadened (see Table 2) to include weight loss and abdominal pain (NICE, 2017a). and leading to a dramatic increase in referrals at the acute trust (from 1500 patients in 2015 to 3500 patients in 2017). The impact of this has been two-fold; first, the expansion of the criteria has led to an increase in the identification of non-colorectal or incidental pathology, such as ovarian, respiratory or renal cancers. This requires robust systems for referring between specialties within the acute trust and co-ordinating appropriate MDT discussions alongside organising any necessary further investigations.
| Patient characteristics: |
Source: National Institute for Health and Care Excellence, 2017a (updated 2015 guideline)
Second, business cases were submitted for additional clinical nurse specialists who could be developed to expand the service predominantly delivered by three existing specialist nurses. The addition of three new team members meant that the majority of clinics were staffed by the nursing team, and medical staff were relied on solely to fill gaps in the service as they arose.
Presentations from the bowel 2WW team have been given at the RCN Centenary (November 2016, London), Association of Surgeons of Great Britain and Ireland conference (May 2016, Belfast) and, more recently, at the Nurse Clinics conference (November 2018, London). Peer feedback from the Nurse Clinics conference was very positive, with a variety of specialties expressing an interest in emulating our service. The team has also recently been approached by several colorectal teams from different hospitals out of county, for advice and support to enable them to set up their own clinics.
Further changes to NICE guidelines (NG12) in 2017 set about achieving early diagnosis through the introduction of the quantitative faecal immunohistochemical test (qFIT) for patients who are considered low risk (but not ‘no risk’) for bowel cancer. (NICE, 2017a). This test uses antibodies specific to human haemoglobin to detect small amounts of blood in a stool sample and, although still subject to false positive results, is considered more reliable as a diagnostic indicator than the previous faecal occult blood tests (NICE 2017a). The acute trust is not equipped to carry out FIT so samples are sent directly from primary care to an out-of-county trust, which is able to support the service. GPs can then refer patients to the bowel 2WW service for patients who have a result equal to or more than 10 micrograms of haemoglobin per gram of faeces (NICE, 2017b).
Referrals from local primary care with positive qFIT noted only started to appear in late 2018, in smaller numbers than were expected, but this may just be a slow start while surgeries put together their own protocols. There may also be a poor return rate when asking patients to carry out stool sampling. This will need further study.
Conclusion
A nurse-led 2WW bowel service has proven to be an effective and efficient way to deliver capacity, and achieve consistent results alongside high levels of patient satisfaction. Fundamental to this process are strict protocols and standard operating procedures that adhere to the necessary governance structures to ensure that the safety of patients and staff is maintained. One thing is certain:, the demand on 2WW service provision ill continue to increase and there is a fundamental need for a flexible forward-thinking approach to meet this pressure. The ideal outcome would be that the nurse team will continue to expand, with a view to removing any reliance on medical colleagues. The authors hope that they can provide support and advice for other teams or specialties who wish to adopt this approach to escalating demand.