

Awound is an interruption in the normal configuration and function of the integumentary and soft tissue architecture, resulting from a variety of mechanisms and underlying causes. Wounds can persist over time without adequate re-epithelialisation, and are considered hard-to-heal if they have not healed with 6 weeks (Jirawitchalert et al, 2022). This type of wound can lead to complications for the patient, such as chronic pain or infection, as well as having psychological and social consequences. The majority of hard-to-heal wounds are associated with conditions such as venous insufficiency, peripheral arterial disease, peripheral neuropathy or poorly progressing surgical wounds. For successful management, it is essential to diagnose the cause of poor healing accurately, initiate timely treatment and provide specialist care based on the characteristics of the wound.
However, in some cases the healing process can take many months or may not even be completed. Hard-to-heal wounds therefore present both a diagnostic and therapeutic challenge for health professionals, particularly dermatologists and community and surgical nurses (Lindholm and Searle, 2016). In this context, punch grafting is a technique that in recent years has gained increasing interest: as is evidenced by the literature, it is a complement to conventional care and treatment, which is designed to accelerate the healing of hard-to-heal wounds and reduce associated pain.
Dermatologists are commonly consulted with regard to skin tumours, which are associated with significant morbidity and mortality if not diagnosed and treated in a timely and appropriate manner. When immediate closure after excision is not possible, the injury can be repaired by flap or graft reconstruction. Alternatively, delayed closure by secondary intention may be considered: this will depend on the wound's location on the body, the patient's characteristics, or in patients where part of a flap or graft has succumbed to necrosis (Conde-Montero et al, 2023).
Solutions
Healing by secondary intention can be augmented with punch grafts. This technique involves using small, split-thickness skin grafts (STSGs), which consist of the epidermis and part of the dermis, to promote epithelial tissue growth and reduce patient discomfort. These superficial grafts can be obtained from a donor site using a punch, curette or scalpel, and then placed onto the ulcer area or surgical injury to promote healing. There is evidence showing that in some instances skin grafting can improve wound healing and reduce chronic pain (Conde-Montero et al, 2020a; García-Madrid et al, 2023), and it has a high level of acceptance among patients. It is a simple and cost-effective procedure that can be performed within the examination room.
Obtaining punch grafts
First, it is important to ensure that the wound bed is properly managed prior to applying the graft. This will facilitate the successful engraftment of the STSGs. An optimal wound bed is therefore one that is clean, that has granulation tissue and no devitalised tissue, and shows no evidence of infection. However, even when the wound micro-environment is not optimal, STSGs can be useful. Even in cases where skin grafts do not adhere to the wound bed, they release growth factors and cells that will promote healing (Conde-Montero et al, 2020b).
If the wound bed and wound conditions are suitable, the patient is called in for a consultation and the procedure is performed on an outpatient basis under local anaesthetic. The first step is to select an optimal donor site on the patient's body from which to harvest the STSGs. The site that is most frequently selected is the anterior thigh.
After infiltration of local anaesthetic, such as mepivacaine or lidocaine, with or without bicarbonate and adrenaline, the STSGs are harvested using a scalpel, punch or curette. Each STSGs will have a diameter of 4–8mm. When taking a punch graft the correct depth is reached when homogeneous punctate haemorrhages, secondary to rupture of the small vessels of the superficial dermal plexus, are observed.
The collected STSGs are carefully placed directly onto the wound bed a few millimetres apart. An interphase dressing (silicone mesh) is then applied on the area, followed by a calcium alginate dressing over this. Finally, gauze is placed over these dressings and a bandage applied to provide compression and encourage adhesion of the STSGs. Local pressure and immobilisation are crucial during the first 4–5 days, in order to fix the graft (Conde-Montero et al, 2020b; Conde-Montero et al, 2023).
Nursing care: understanding the theory
Appropriate and individualised treatment is essential for the success of punch grafting.
Preparation of the wound bed
Prior to the transfer of an STSG, the wound bed must be prepared by debriding it of devitalised tissue, to ensure it is fully cleansed before the grafting procedure. Ideally, the wound bed should be brownish-red in colour, flat and slightly moist. However, in cases where there has been prolonged would healing, it is not uncommon to see excessive granulation tissue on the surface of the wound bed, known as hypergranulation, when a patient arrives for the procedure. The granulation tissue will have been formed in a dysfunctional pro-inflammatory environment that supports increased proliferation of fibroblasts and endothelial cells. The wound bed may have a slightly protruding appearance, be friable (bleed easily), or be deep red in colour. This will impede the ability of keratinocytes to undergo proliferation and horizontal migration, which will ultimately hinder the healing process.
Any hypergranulation in the wound needs to be treated before the transfer of the graft: an effective treatment is the application of silver nitrate that sticks gently to the tissue of the bed. However, this method of chemical debridement can be painful and may cause scarring and a foreign-body reaction and, consequently, treatment with topical steroids to address hypergranulation is increasing (Linneman and Litt, 2022). In a retrospective review, the application of 1% hydrocortisone cream was found to lead to faster wound healing times compared with chemical cauterisation with silver nitrate (Linneman and Litt, 2022).
During the procedure
The wound edges and the STSGs must be protected during the grafting procedure. Dressing changes and debridement of the wound bed by any method – the latter carried out only if absolutely necessary – must be undertaken with great care to avoid damaging the tissue and hindering the healing process. This is because there is a possibility of damaging or tearing some of the STSGs, as well as disrupting the healing process, since a significant proportion of growth factors contained within the wound bed may be lost during debridement.
Dressing changes
The first dressing change is usually recommended 5–7 days after surgery. The layers of dressings should be uncovered carefully and the silicone mesh removed. First, the area needs to be cleansed using saline or an antiseptic solution composed of purified water, undecylenamidopropyl betaine and polyhexanide, and any adhesive residue from the initial dressings must be carefully removed. The nurse will need to assesses the wound characteristics, including the appearance of the wound bed and STSGs, presence or absence of devitalised tissue, and to observe for signs of infection.
At subsequent dressing changes, if the STSGs grafts are taking well, they will appear more pink and purple than they looked at the first dressing change. This will be due to angiogenesis, which occurs from the wound bed to the STSGs in the first few days following graft transfer. However, if a graft has not taken hold, the STSGs will be a yellowish colour. Grafts that have not attached and remain in the dressing should be replaced in the wound bed. During subsequent dressings, the STSGs will become whiter in colour and larger in size, with bridges forming between them. Additionally, the wound bed will become increasingly pink and progressively more white in colour as the re-epithelialisation process advances. The wound can be regrafted as many times as necessary until complete epithelialisation is achieved. This is not uncommon in wounds with an initially suboptimal wound bed.
Until re-epithelialisation has been completed, it is recommended that the patient is reassessed once a week subsequent to the first dressing change. Complete healing may be achieved within a few weeks. From the first few days after STSG placement, patients generally report some or complete alleviation of wound-related pain (Conde-Montero et al, 2020b; Conde-Montero et al, 2023; García-Madrid et al, 2023). Although the mechanism for this after placement of STSGs is not well understood, this may be important as an indicator that the graft is adhering to the bed and, more importantly, pain reduction improves the patient's quality of life.
Donor site assessment
Initial examination and treatment of the donor area can be undertaken on the same day as the assessment and preparation of the recipient site. Assessment and nursing care with regard to the donor site is similar to that for the recipient area.
Case study
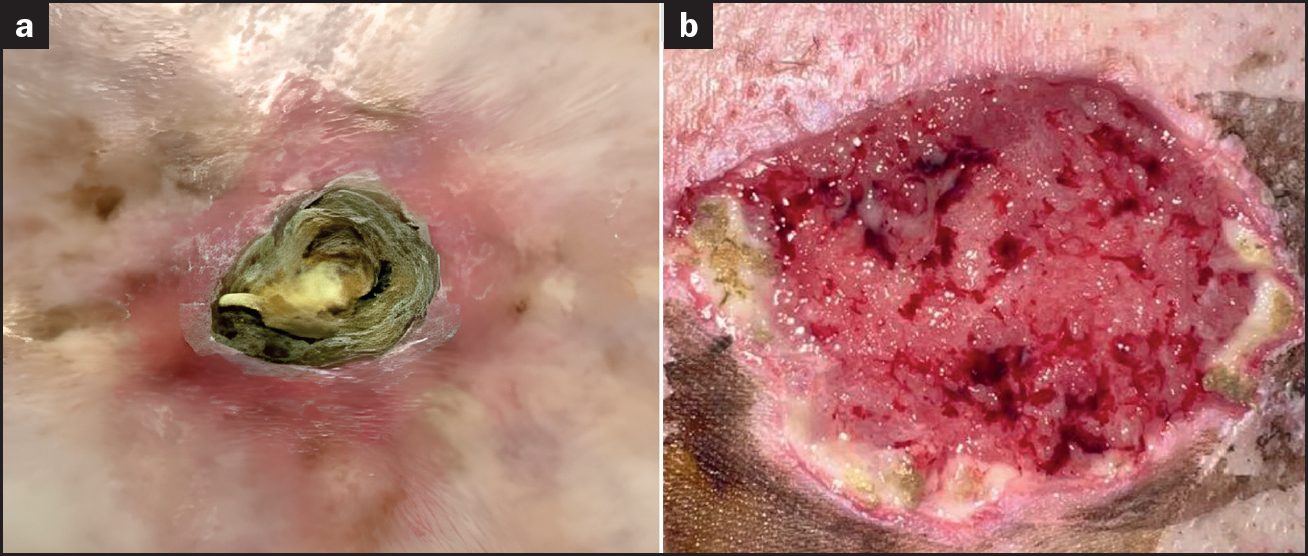
The management of an 82-year-old man with a medical history of hypertension, dyslipidaemia and obesity is illustrative of the process of skin grafting. The patient was referred to the authors’ dermatology outpatient clinic due to a long-standing lesion at the site of a flame burn that he had suffered on his abdomen as a child, which had increased progressively in size over the preceding 6 months and caused pain on palpation. Examination of the patient's abdominal area revealed a lesion of approximately 4cm in size, with erythematous borders and a hyperkeratotic central area over a diffuse whitish scar (Figure 1a).
Tumour removal
Partial removal of the scab disclosed an irregular ulcerated wound bed. A biopsy was taken from the ulcerated surface, with the test results identifying well-differentiated squamous cell carcinoma with clear margins and no evidence of perineural or lymphovascular invasion.
An operation was scheduled to remove the tumour under local anaesthetic and sedation. This was excised with safe margins, but closure of the primary defect was complicated by the rigidity of abdominal skin due to fibrosis resulting from the old burn. As a result, the skin was minimally displaced, making it difficult to perform a skin flap. Undertaking a traditional full-skin graft (partial or full thickness) was not considered a good option because it was considered that there was a high risk of failure due to the surrounding scarred skin. It was therefore decided to leave the wound to heal by secondary intention after removal of the tumour and to apply dressings at periodic intervals until complete re-epithelialisation had occurred.
When the patient came in for his first dressing change 3 days following excision of the tumour, the surgical wound on the abdomen measured 4cm x 3.5cm with no evidence of active bleeding or signs of inflammation or infection. The patient reported moderate pain on palpation (6/10 on 10-point visual analogue scale (VAS)). The wound was cleansed with Prontosan solution and any adherent debris mechanically removed. An alginate dressing, gauze and a compression bandage were then applied. Following assessment of the wound by the nursing team responsible for the patient's wound care and the dermatologist it was agreed that the patient would return in a few days for the application of negative pressure wound therapy using a PICO wound dressing. After 3 weeks, despite the fact that wound healing had progressed well, the diameter of the affected area had decreased only slightly (Figure 1b).
Graft procedure and follow-up care
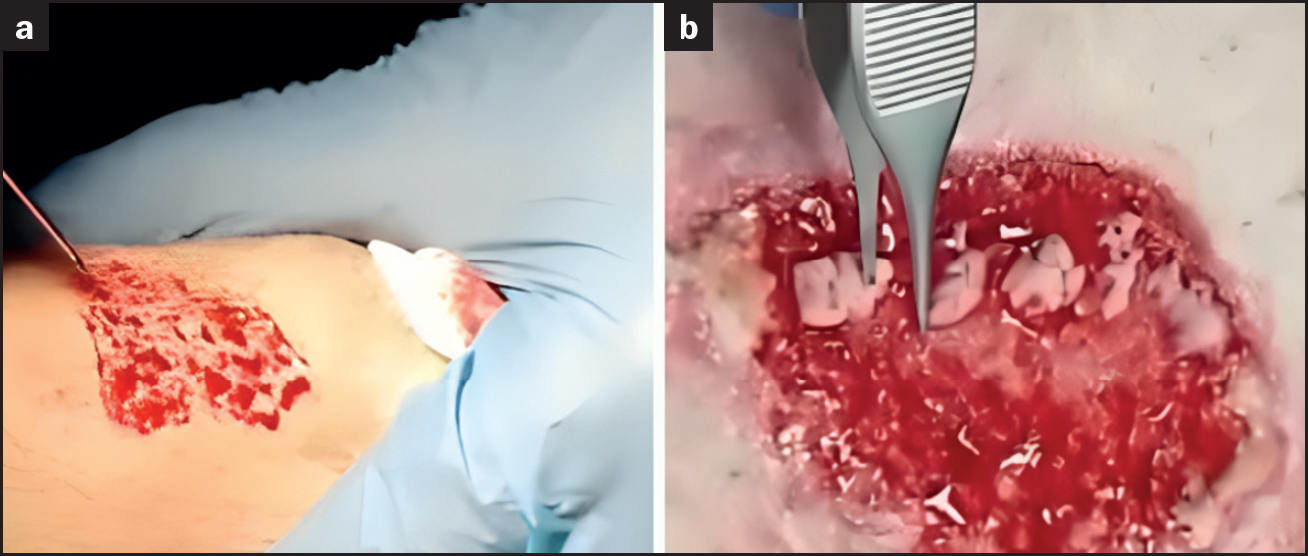
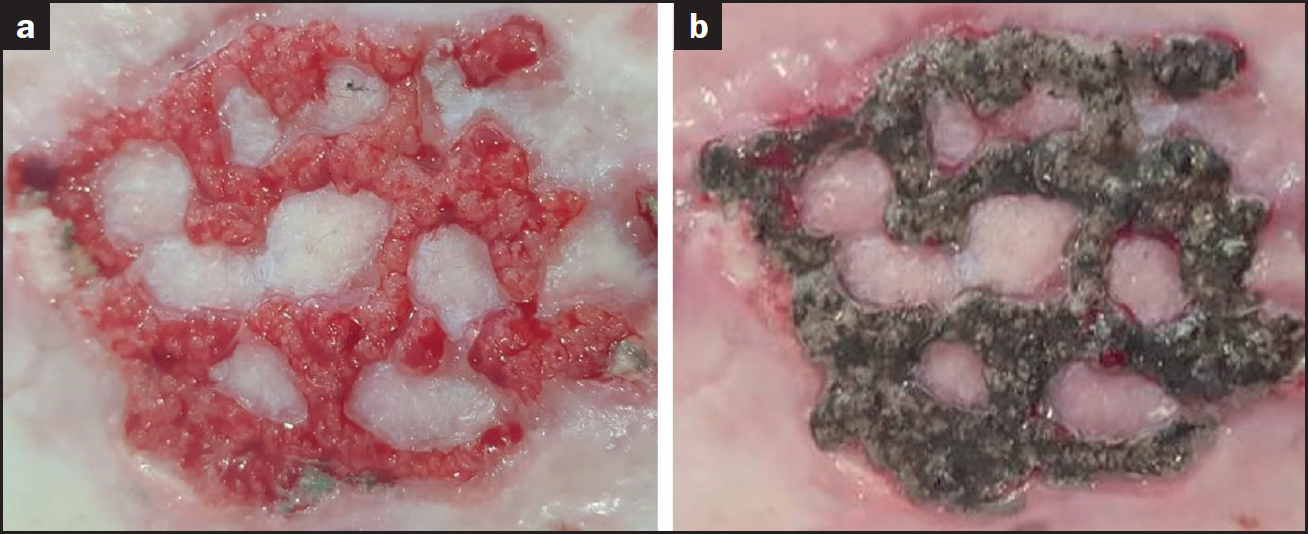
For these reasons, and taking into consideration the condition of the wound bed, it was agreed with the patient to perform the punch graft technique. The anterior aspect of the thigh was used as the donor site, with the STSGs harvested under local anaesthesia (mepivacaine 2%) using a scalpel (Figure 2a). The the grafts were taken down to the depth of the papillary dermis, with characteristic punctate bleeding observed in the donor area. The STSGs were then carefully placed onto the wound bed (Figure 2b), and covered with a silicone mesh interface dressing and an alginate dressing (Figure 3a). A negative pressure wound therapy dressing was then applied to promote adhesion to the wound bed. The donor site, which was roughly 3cm x 2cm in size, was also dressed with an alginate dressing and bandage.

After 7 days, the patient came in for his first follow-up assessment. The STSGs were found to be in good condition with a pinkish discolouration indicating adequate attachment to the wound bed (Figure 3b). A new interphasic dressing, alginate and compression dressing were applied to both wounds, donor and recipient. Pain was virtually absent (VAS: 1/10).
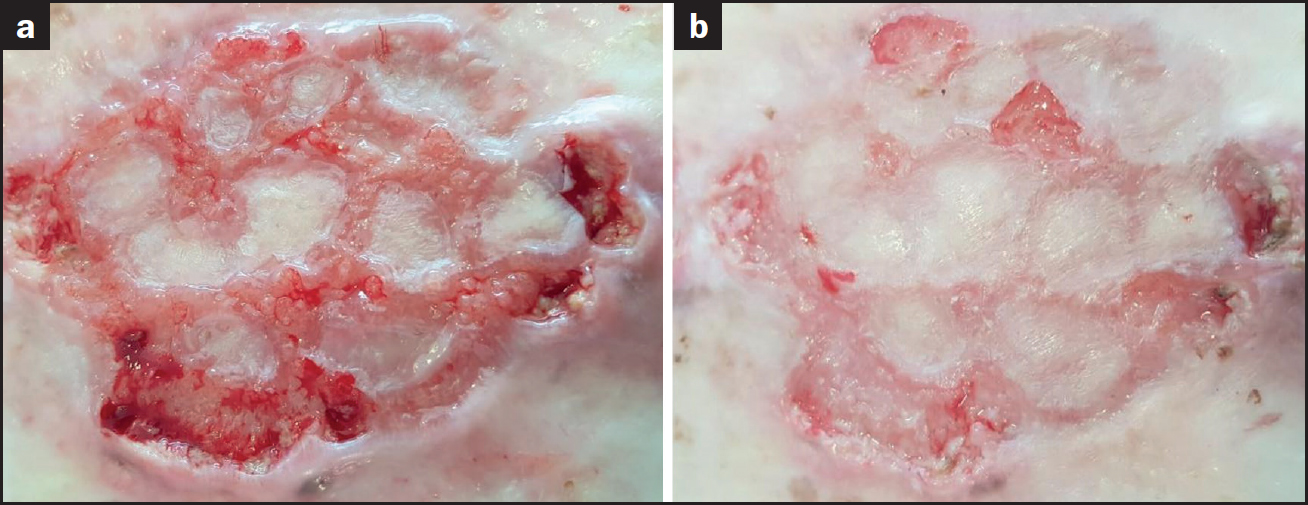
At the next assessment, the STSGs were whitish in colour and had begun to grow slightly (Figure 3c). Examinations at subsequent follow-up visits revealed hypergranulation and it was decided to carefully cauterise the excess granulation tissue (Figure 4a). A silver nitrate rod was used to cauterise excess granulation on the wound bed, to ensure that the STSGs protruded sufficiently into the wound margins (Figure 4b). The patient continued to attend the clinic once a week. The progression of the wound was favourable, with hypergranulation requiring only one further treatment (this time, with the application of a medium-strength topical corticosteroid), and the wound gradually re-epithelialised (Figure 5a).
Both wounds were dressed weekly in a similar manner, although the final dressings did not include alginate in the donor and recipient sites. The donor site required a silicone mesh and a compression dressing for the first few weeks only, and a polyurethane foam dressing was subsequently applied to protect the wound and absorb exudate.
Healing was virtually complete 7 weeks after placement of the STSGs (Figure 5b). The patient was advised to continue with dressing changes at his health centre until complete healing had occurred. The patient is currently undergoing regular follow-up at the authors’ clinic every 6 months with no evidence of local or lymph node recurrence of his tumour.
Benefits of punch grafting
This clinical case has illustrated the effectiveness of performing punch grafting in a hard-to-heal wound following surgery for a skin tumour. The procedure has been described in detail, along with the appropriate dressings, which must be adapted according to the progress in healing of the patient's wound.
In the case of the case study patient, his wound re-epithelialised completely within a few weeks, with no associated complications in the graft or donor areas. Of particular note was the rapid resolution of pain within a few days of onset. Punch grafting has been used mainly in patients with chronic lower extremity ulcers, particularly of venous, arterial, hypertensive and diabetic aetiology (Groening et al, 2017). There are fewer case reports of its use in surgical wounds healing by secondary intention, as in the case reported in this article (Seo et al, 2016).
Considerations
Punch grafting is a simple technique that can be performed on an outpatient basis with low patient morbidity. Furthermore, when used in selected cases of surgical injury, where closure by secondary intention is being considered, it can be more costeffective than carrying out a new surgical procedure to close the injury or reduce the number of patient visits to the nurse for wound dressing changes.
Punch grafting is an emerging technique that, in the view of the authors, will play an increasingly important role in the treatment of complex wounds in the coming years. It has also been employed in the treatment of atrophic acne scars and vitiligo. In the latter case, it has been used for decades and there is growing evidence to support its use. It is an exciting relatively new therapy. When used for vitiligo, punch grafting is often combined with phototherapy to accelerate repigmentation of grafted areas. A recent meta-analysis (Ju et al, 2021) of 1631 patients with vitiligo from 19 studies showed a repigmentation rate greater than 50% in 71% of patients and greater than 90% in 45% of cases. A disadvantage of punch grafting is the need to make a second wound to harvest the STSGs. This means that dressings must be applied to this site as well. There is also a risk of infection at the donor site. In addition, it can sometimes lead to the development of unaesthetic or hypertrophic scarring (Ju et al, 2021).
The role of the nurse in the management of these patients is fundamental. This includes nursing input and assessment before, during and after the punch graft technique. The nurse's intervention starts with the selection of appropriate dressings in the weeks before the punch graft procedure is performed. The aim is to leave the wound bed in the best possible condition, with or without prior application of negative wound pressure therapy (Martín-Alcalde et al, 2022; Guisado-Muñoz et al, 2019).
During the punch graft procedure, the doctor and nurse are responsible for the removal and placement of the grafts into the wound bed. Once the procedure has been completed, it should be explained to the patient the importance of not removing the dressings until the following week. The patient should also be advised to rest to allow the STSGs to take hold properly. When the patient returns for the subsequent dressing change, the nurse carries out an individualised assessment. The characteristics of the wound must be considered and acted upon, if necessary. This process is essential to the success of STSGs.
Patients will require visits to see the nurse once a week for treatment of the wounds at both the donor and recipient sites. Wound healing time will depend on wound characteristics, location and other factors, and is usually between 2 and 10 weeks from the time of STSG placement.
Conclusion
In the authors’ opinion, punch grafting should be considered as an alternative for specific dermatological surgical wounds. For example, the technique may be a good option for surgical wounds where primary closure has failed, where a large amount of skin needs to be mobilised for a large flap or graft, or where closure by secondary intention is being considered. To perform the technique correctly requires a trained clinician and the support of a nursing team who is knowledgeable about the selection and correct application of appropriate dressings to suit the wound conditions. Further studies are required to provide more evidence to support the use of punch grafting in postoperative wounds.
Key points
- Punch grafting is a relatively straightforward technique that can be performed on an outpatient basis
- It is a useful technique for accelerating the healing of hard-to-heal wounds and reducing a patient's pain
- The patient will require regular nursing care following the transfer of the graft, with the application of appropriate dressings, depending on the condition of the wound at the recipient site
- Punch grafting has been used successfully in hard-to-heal wounds of various aetiologies. The authors have demonstrated its efficacy in accelerating the healing of surgical wounds following skin excision
CPD reflective questions
- Consider whether punch grafting could be a promising option to heal surgical skin injuries
- Should nurses working in dermatology or plastic surgery services be trained more specifically in this technique?
- Can you think of any recent developments in the performance or follow-up of the technique described in this article that could further improve the results of the technique?