
Nursing is a highly demanding profession that often results in intrusion of work into family life to a point where work and family demands affect one another (Abdul Rahman et al, 2017). Inter-role conflict has been studied since the 1960s, when Kahn et al (1964) observed that incompatible institution demands have adverse effects on personality characteristics and interpersonal relationships. Kahn et al (1964:20) observed inter-role conflict as a form of conflict in which:
‘Role pressures associated with membership in one organization are in conflict with pressures restricting from membership in other groups.’
Greenhaus and Beutell (1985) expanded on this theory and defined it in the context of work and family as a type of inter-role conflict that occurs as a result of incompatible role pressures from the work and family domains. They explained that work-family conflict could take three forms:
Netemeyer et al (1996) further elaborated and explained that work-family conflict could occur as a form of family-to-work conflict (where roles in the family affect roles at work) or work-to-family conflict (where roles in the family are affected by roles at work).
Research studies have demonstrated that nurses faced difficulty balancing their family role with their responsibilities at work due to intense work pressure, leading to lowered commitment to work and the organisation (Hatam et al, 2016), as well as increased intention to leave for better working conditions or to leave the profession altogether (Nadi and Hazeghy, 2011). In view of the fact that ‘family comes first’ in many societies, it is important to explore and fully understand the outcomes of an adverse work-family balance (Sharma et al, 2016). The relationship of work-family conflict towards job satisfaction and health status is under-reported in the current literature. Poor job satisfaction and increased sickness absences impact the whole organisational performance and lead to a host of financial, social and quality-of-care issues. Therefore, this study aimed to explore the relationship of work-family conflict on the health status and job satisfaction of nurses.
Methods
Study design, population and sample
A cross-sectional study was conducted using a self-administered questionnaire involving nurses from the largest referral hospital in Brunei. The eligibility criteria were nurses working in high-dependency settings (emergency department and critical care settings) and general settings (male/female medical wards, male/female surgical wards, neurology and orthopaedic wards), and not on leave or long-term absence. A minimum sample size of 385 is required to achieve the following parameters: power=80% and alpha=0.05. A total of 500 questionnaires were distributed to account for attrition and withdrawal (Naing et al, 2006).
Data collection procedure
There was no direct contact between the researchers and the respondents in the study. The eligible sample were identified by the gatekeeper, ie the head of department of each unit. All of the participants received a sealed package containing an envelope for returning the questionnaire, the questionnaire, participants' information sheet and two copies of the consent form. Participants would then return one copy of the signed consent form and the completed questionnaire in the envelope provided within a week. One week was allocated for the participants to respond to ensure that they would have ample time.
Data collection instrument
Data were collected through a self-administrated questionnaire. The questionnaire consisted of two sections. The first consisted of participants' sociodemographic information. This included: age, gender, marital status, number of years working as a nurse, body mass index and smoking status. The second section collected data on work-family conflict, self-rated health and job satisfaction, which was measured using the Copenhagen Psychosocial Questionnaire II (COPSOQ II) developed by the National Research Centre for the Working Environment in Denmark (Pejtersen et al, 2010).
Data analysis
Descriptive statistics were computed with an accompanying 95% confidence interval using a normal approximation method. Independent t test, one-way ANOVA, chi-square test and Pearson's correlation were used in subgroup analysis to compare sociodemographic factors with study outcomes, as well as the relationship between study outcomes (work-family conflict, self-rated health and job satisfaction). Higher Spearman's correlation coefficient rho statistics indicate a stronger association (Kellar and Kelvin, 2013). Higher mean scores of study outcomes correspond to higher effects of the respective variable. All statistical procedures were conducted using R-v.3.3.3. A P-value less than 0.05 is considered statistically significant (two-sided).
Ethical considerations
The institutional research ethics committee at the Ministry of Health approved the study protocol (UBD/IHS/B3/8). Written consent was obtained from the participants before they completed and returned the questionnaire. No identifying information was recorded during data entry and analysis. All records were discarded 1 year after completion of the study.
Results
A total of 426 respondents returned their completed questionnaires and were included in this study (85.2% response rate). Table 1 describes the sociodemographic factors of the nurses working in the general and high-dependency units. Female participants made up 72.3% (95%; CI: 67.7, 76.4) of the sample; 65.5% (95% CI: 60.7, 70.0) of the participants were married. Mean age was 37.2 (±8.7) years, with an average of 11.7 (±7.3) years of working experience. The majority of respondents were non-smokers (92.5%); however, 41.8% of them were overweight and 25.1% were obese.
| n | Percentage (%) | Mean | (SD) | (95% CI) | |
|---|---|---|---|---|---|
| Age | 37.2 | (8.7) | (36.4, 38.1) | ||
| Gender | |||||
| Male | 118 | (27.7) | (23.6, 32.2) | ||
| Female | 308 | (72.3) | (67.7, 76.4) | ||
| Marital status | |||||
| Married | 279 | (65.5) | (60.7, 70.0) | ||
| Single | 147 | (34.5) | (30.0, 39.3) | ||
| Work experience (years) | 11.7 | (7.3) | (11.0, 12.4) | ||
| Body mass index | |||||
| Normal | 141 | (33.1) | (28.7, 37.8) | ||
| Overweight | 178 | (41.8) | (37.1, 46.6) | ||
| Obese | 107 | (25.1) | (21.1, 29.6) | ||
| Smoking status | |||||
| Yes | 32 | (7.5) | (5.3, 10.5) | ||
| No | 394 | (92.5) | (89.5, 94.7) | ||
| Settings | |||||
| High-dependency | 201 | (47.2) | (42.4, 52.0) | ||
| General | 225 | (52.8) | (48.0, 57.6) | ||
n=frequency, SD=standard deviation, CI=confidence Interval
Table 2 represents the relationship between sociodemographic factors and study outcomes, including work-family conflict, self-rated health and job satisfaction. The results revealed that increasing age and being married were significantly related to higher job satisfaction (P<0.001). In addition, those who did not smoke reported significantly higher job satisfaction (P=0.005) and better health (P<0.001). Nurses working in the general setting reported experiencing significantly higher work-family conflict compared to nurses working in high-dependency settings (P<0.001). Despite this, nurses working in the general setting reported significantly higher job satisfaction and better health status (P<0.001). No significant relationship was detected between study outcomes and gender, BMI and years of working.
| Work-family conflict | Self-rated health | Job satisfaction | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | (SD) | P-value | Mean | (SD) | P-value | Mean | (SD) | P-value | |
| Age (years) † | 0.08 | - | 0.104 | 0.09 | - | 0.060 | 0.26 | - | <0.001 |
| Gender ‡ | |||||||||
| Male | 2.04 | (0.8) | 0.066 | 3.07 | (1.1) | 0.070 | 2.36 | (0.8) | 0.093 |
| Female | 2.23 | (0.9) | 2.85 | (1.1) | 2.49 | (0.8) | |||
| Marital status | |||||||||
| Married | 2.23 | (0.9) | 0.116 | 2.94 | (1.2) | 0.440 | 2.36 | (0.7) | <0.001 |
| Single | 2.08 | (0.8) | 2.85 | (1.0) | 2.63 | (0.8) | |||
| Work (years) † | 0.01 | - | 0.764 | 0.05 | - | 0.313 | 0.05 | - | 0.304 |
| BMI § | |||||||||
| Normal | 2.17 | (0.7) | 0.320 | 3.06 | (1.0) | 0.278 | 2.56 | (0.8) | 0.292 |
| Overweight | 2.26 | (1.0) | 2.77 | (1.2) | 2.36 | (0.7) | |||
| Obese | 2.04 | (0.9) | 2.94 | (1.2) | 2.48 | (0.9) | |||
| Smoking status ‡ | |||||||||
| Yes | 2.08 | (0.8) | 2.28 | (0.8) | 2.09 | (0.7) | |||
| No | 2.18 | (0.9) | 0.522 | 2.96 | (1.1) | <0.001 | 2.49 | (0.8) | 0.005 |
| Settings ‡ | |||||||||
| High-dependency | 1.81 | (0.7) | 2.20 | (0.9) | 1.94 | (0.6) | |||
| General | 2.50 | (0.9) | <0.001 | 3.54 | (0.9) | <0.001 | 2.92 | (0.6) | <0.001 |
=Pearson's correlation (rho)
=independent t test
=one-way ANOVA
SD=standard deviation
BMI=body mass index
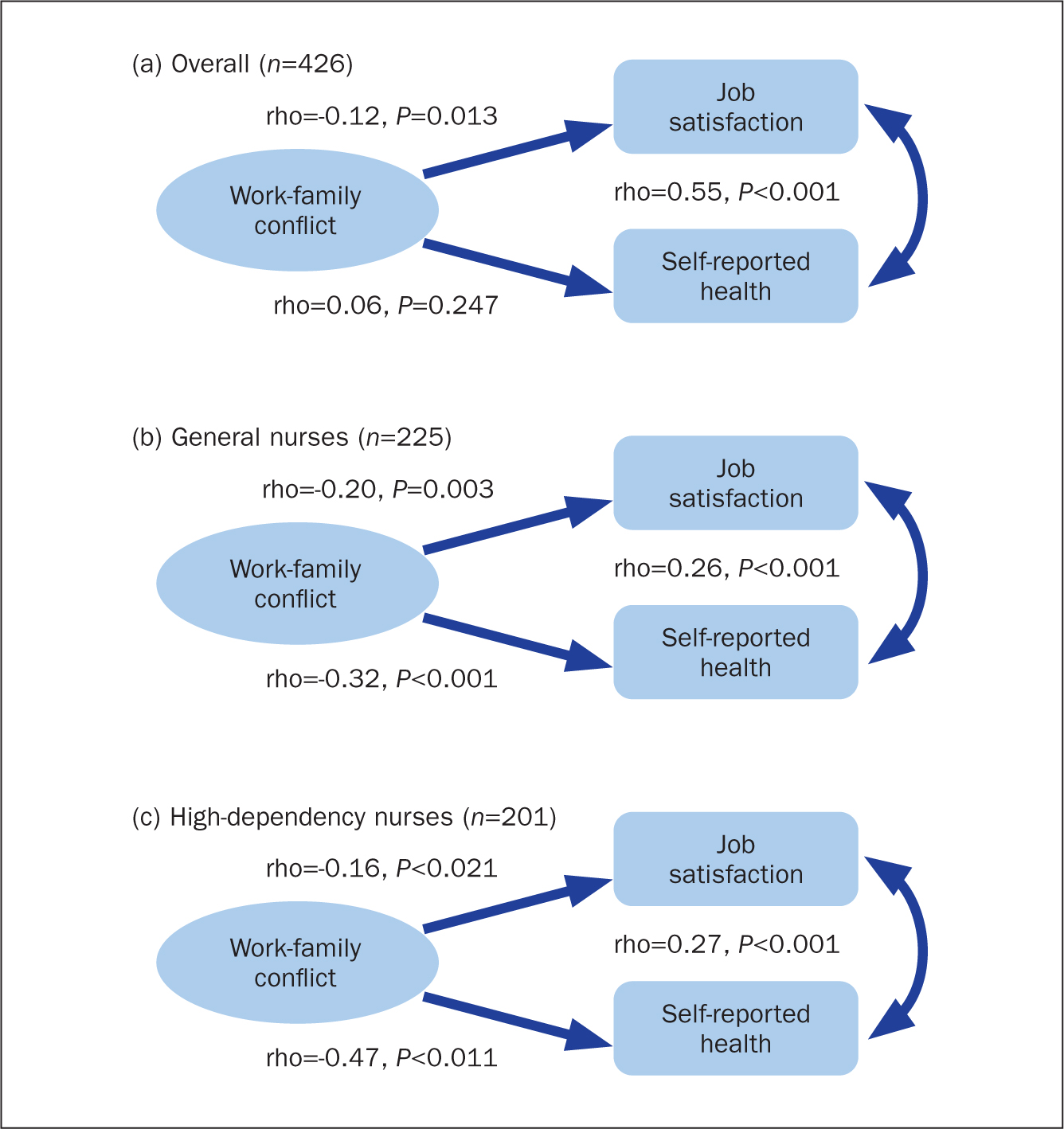
Figure 1 illustrates the correlation between work-family conflict, job satisfaction and self-rated health. The results revealed that there was a significant negative relationship between work-family conflict and job satisfaction. It was observed that higher work-family conflict corresponded to lower job satisfaction, albeit the strength of this relationship was weak (rho=–0.12). Although there was no statistical significance in the overall relationship between work-family conflict and self-rated health, there was significance by settings. It was observed that this relationship was stronger in high-dependency nurses, where increase in work-family conflict had a significant reduction in health status (rho=-0.47). Furthermore, there was also a significant positive relationship between job satisfaction and self-rated health. It was observed that better health status corresponded to higher job satisfaction, and this relationship had moderate magnitude (rho=0.55).
Discussion
To the best of the authors' knowledge, this is the first study examining the relationship between work-family conflict, self-rated health and job satisfaction among nurses in Brunei. First, the study found that nurses who were married experienced higher work-family conflict and lower job satisfaction. Using the theory of Greenhaus and Beutell (1985) to understand this phenomenon, work-family conflict could be the pressure of work inhibiting nurses from participating in the responsibilities of family life or vice versa. This conflict could be derived from married nurses possibly have greater responsibilities (such as child care and care for older family members), resulting in difficulties in balancing family roles and roles at work. It is also possible that lower job satisfaction could be contributing towards this conflict since reduced job satisfaction is significantly related to lack of job control, high job demand and stress, and poor staff management and inadequate resources (Ding et al, 2018; Khamisa et al, 2015). Despite this, those who were married had significantly better health status. This could be attributed to stronger emotional, physical and familial support from their spouse, children and close family members for better health and health-seeking behaviours, which leads to better quality of life and satisfaction (Sharhraky et al, 2011).
The present study also showed that an increase in work-family conflict results in significantly reduced job satisfaction and health status. This is particularly relevant for work-induced conflict where the working environment adversely impacts nurses, such as when work impinges on family time (Khamisa et al, 2017). A less conducive working environment could lead to a nurse being overweight or obese and lead to an increase in smoking (Ioannou et al, 2015), alcohol consumption (Trybou et al, 2014) and musculoskeletal disorders (Abdul Rahman et al, 2017). Those engaged in rotational and night shift work, which most nurses are exposed to, have a higher prevalence of these problems (Miranda et al, 2015; Nea et al, 2015).
In terms of implications for practice, this study provides evidence that healthcare and nursing administrators and policymakers can use to foster effective strategies and interventions supporting the balance of nurses' work and family life. Developing a robust electronic self-rostering system to cater for supply-and-demand changes for assigning shifts could be a possible way to ameliorate work-driven conflict (Drake, 2014). However, the focus should be on transformational and organisational changes that address work-family conflict and related issues and promote an optimal working environment (Kelly et al, 2014).
Limitations
The results of this study should be interpreted within its limitations. The strength of this study lies in the adequate sample power to detect significance at 5% precision, following the standard in scientific research, therefore findings from this study are generalisable to the study population. However, the use of a questionnaire is subject to reporting and recall bias. In addition, this study investigated work-family conflict on a general scope and further studies should have an in-depth exploration of the nature of this conflict. Future studies could also employ prospective study methods with observational data to strengthen evidence to better inform nursing policymakers and management.
Conclusion
Work-family conflict impacts nurses' job satisfaction, health and wellbeing, as well as compromising efficiency, performance and quality of patient care, which affects the entire healthcare organisation. Further studies incorporating transformational and organisational strategies are needed to seek solutions that encapsulate all related issues on work-family conflict.