
The process of conducting a patient consultation and performing a subsequent clinical assessment has historically been termed ‘the most powerful and sensitive and most versatile instrument available to the physician’ (Engel, 1973). Despite the rapid growth of healthcare technology, this remains the case today. A skilled advanced clinical practitioner (ACP) in this area has the potential to make a significant contribution to several fundamental outcomes: patient satisfaction, patient concordance with prescribed therapies/interventions, overall diagnostic accuracy and overall patient outcomes. Evidence suggests that, by conducting a high-quality medical history alone, 60-80% of the relevant information to form a diagnosis can be ascertained (Peterson et al, 1992; Roshan, 2000). The overall aim is to identify symptoms and physical manifestations that represent a final common pathway of a wide range of pathologies, which may be highly suggestive or even pathognomonic of one such pathology, or multiple concurrent pathologies.
Communication
Communication with patients is key to all aspects of clinical practice. Seminal NHS frameworks and policy drivers place effective communication at the core of providing a person-centred approach in health and care (Health Education England (HEE) 2017; HEE et al, 2017; NHS England 2019a; 2019b). Communication skills are consequently core strands of ACP training and ongoing professional development. Effective communication with patients can lead to improvement in both treatment quality and safety metrics (Scalise, 2006; Krug, 2008; Brock et al, 2013); conversely, poor communication has been highlighted as one of the main concerns that lead to complaints to the Parliamentary and Health Service Ombudsman (2020a; 2020b).
In order to develop effective ACP-patient relationships we must consider some of the fundamental principles of effective/therapeutic communication within the healthcare setting, such as patient health literacy, cultural understanding and language barriers. However, there are other aspects that could potentially have an impact (Table 1).
| Deciding to consult a doctor | Patient's perceptions of: |
| Triggers to consultation |
|
| Consultation environment |
|
It is undeniable that therapeutic communication is complex, however several constructs and consultation frameworks have been proposed over the decades to aid the clinician/practitioner in working with patients as partners. The development of these frameworks has more recently led to validated scoring systems such as the Global Consultation Rating Scale (Burt et al, 2014), which have been produced to assess the communication quality of consultations.
Constructs
Mehay (2012) has proposed several constructs or ‘mental grids or frameworks’ through the use of mnemonics that can aid communication with patients in specific, sometimes challenging, situations (Table 2).
| Breaking bad news | Dealing with an angry patient | ||
|---|---|---|---|
| A | Anxiety: acknowledge | A | Avoid confrontation |
| K | Knowledge: what do they already know? | F | Facilitate discussion |
| I | Information: how much info do they want? Keep it simple, avoid overload | V | Ventilate feelings |
| S | Sympathy + emotional management | E | Explore reasons |
| S | Support: ask what would help | R | Refer/investigate |
| S | Summarise strategy and key points | ||
| Conflict situations | Ethical considerations | ||
| D | Disagree | A | Autonomy (patient): be fair (justice) |
| A | Agree | B | Beneficence |
| N | Negotiate a compromise | C+C | Consent + confidentiality |
| C | Counsel | D | Do not lie |
| E | Educate | E | Everybody else (society vs individual): virtue, duty, utility and rights |
| R | Refer to third party | ||
Consultation models/frameworks
During any consultation there will be a varying degree of information sharing, and the practitioner will inevitably have a number of tasks that need to be performed. In order to maximise the efficiency and efficacy of the consultation, a number of models or frameworks have been proposed over the decades. These can be task oriented, clinician centred, behaviour centred and patients centred. Although most models have been developed for use within the primary care/GP setting, they are arguably also applicable to secondary care and tertiary care settings, with adaptation as necessary.
All consultation frameworks share the common task of obtaining a medical history; however, Mehay (2012) classifies them as differing in three ways:
Mehay (2012) also proposes a simple diagram that details the degree to which a selection of the existing frameworks differ, in terms of their focus on the three aforementioned classifications However, there have since been two further evidence-based frameworks produced by Norman and Tesser (2015) and Jack et al (2018), which further enhance the balance between all three of Mehay's (2012) classifications.
Consultation frameworks promote a thorough and safe approach to the information gathering, information processing and subsequent outputs of the patient-practitioner consultation. Practitioners may differ as to which framework they use and indeed how they adapt it into their own practice, which will largely depend on the nature of the encounter. The Calgary-Cambridge Guides (CCG) and the enhanced CCG (eCCG) (Kurtz et al, 1996; 2005; Kurtz et al, 2003) have become the dominant models used for teaching consultation skills in advanced practice and medical training programmes, and for subsequent use within the clinical arena.
Frameworks and disease prevention
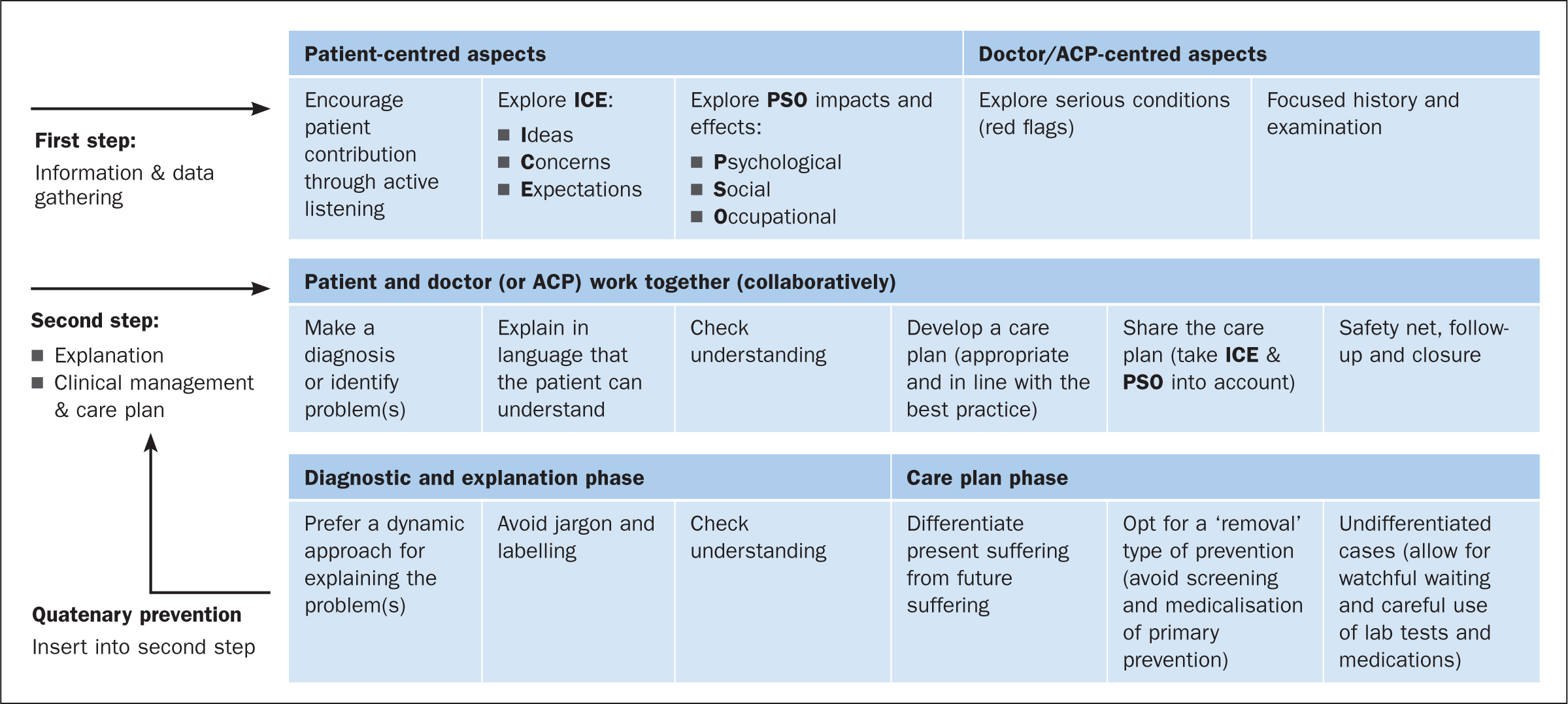
The CCG and eCCG (Figure 1) are evidence-based frameworks that enable the ACP to tailor the medical consultation by improving 71 communication skills and behaviours. Norman and Tesser (2015) have proposed a further enhancement to the eCCG, which has been used as an organisational matrix to insert the theory of quaternary prevention (CCG+QP) (Figure 2). Kuehlein et al (2010) defined quaternary prevention (QP) as ‘an action taken to identify a patient at risk of over-medicalization, to protect him from new medical invasion, and to suggest to him interventions which are ethically acceptable’, a definition that has since widely been accepted in both health care and academic literature. Martins et al (2018) have expanded on this definition to include ‘refraining from providing therapy that has not been adequately assessed in a randomized controlled trial with low risk of bias’.

QP adds a further dimension to the existing public health literature surrounding the principles of primary, secondary and tertiary disease prevention. Much like the plethora of consultation frameworks, the QP literature focuses primarily on it application in the general practice/primary care arena. However, ACPs within all sectors are presented with significant opportunities to protect their patients from potential iatrogenic harm as a consequence of overmedicalisation. QP ‘should be present in the mind of every healthcare professional when they suggest an intervention to one of their patients’ (Martins et al, 2018).
Aspects of obtaining a medical history
As mentioned, obtaining a medical history is embedded within the background information section of the eCCG (Figure 1). A comprehensive history commonly consists of several components, each of which has a variety of mnemonics that can be used to aid the practitioner to elicit salient information at each stage (Table 3) (Hocking et al, 1998; Rothman and Kulkarni, 2008; Talley and O'Connor, 2017; Innes et al, 2018; Bickley, 2020).
| Components of the adult health history | Data | Mnemonics | ||
|---|---|---|---|---|
| Identifying data/personal information |
|
|||
| Presenting complaint (PC) |
|
O Onset of complaint |
OR |
OR (FOR PAIN) |
| History of presenting complaint |
|
|||
| Past medical history (PMH) |
|
Common illnesses with associated morbidity and mortality: |
||
| Drug history |
|
D Doctor: medications prescribed by a registered health professional |
||
| Family history |
|
FAMILY Multiple affected siblings or individuals in multiple generations (absence does NOT rule out genetic causes) |
||
| Social history |
|
W What do you do? Note chemical, dust, animal, paint and disease exposure |
||
| Review of symptoms |
|
M Musculoskeletal: bone and joint pain/muscular pain |
||
The traditional history-taking format meets many challenges in the time-critical situation, and the nature of these dynamic situations often means that a quick, focused history is required. The mnemonic ‘AMPLE’, originally developed for use in the context of trauma (Zemaitis et al, 2020), may be applied to quickly obtain pertinent information:
Clinical assessment: aspects of physical examination
Although a well-conducted, thorough physical examination requires a systematic approach, it does not always require a full examination for each body system. Salient points from the initial consultation stage may guide the clinician as to the focus of a general examination. Future issues of the ACP series will cover the body's systems, such as the cardiac and endocrine systems, in more depth, but the process of performing a full physical examination, along with a non-exhaustive list of potential examination findings, is presented below. Again, there may be time-critical situations in which this approach is not appropriate, and these situations lend themselves to an ABCDE (airway, breathing, circulation, disability and exposure) approach (Resuscitation Council UK, 2015).
The following is a guide to performing a systematic examination, but this is not an exhaustive list:
General survey
Vital signs
Hands and nails
Arms
Head and neck
Thorax
Abdomen
Lower limbs
Conclusion
Consultation and clinical assessment are fundamental skills of the ACP role, the process of which is complex and requires an array of underpinning knowledge in physiology, pathophysiology and theories of effective communication within the healthcare setting. There are multiple frameworks to guide the process, not all of which will be suitable for many specialist areas in which ACPs practice. There are multiple opportunities throughout the clinical consultation process in which ACPs can engage with their patient population, in order to work in partnership to enhance primary, secondary and tertiary prevention of disease and the healthcare intervention burden. A number of newer consultation frameworks now address quaternary prevention; however their use in the secondary and tertiary care settings is yet to be evaluated.