
Stable, reliable venous access is required to administer intravenous fluids and medications as well as to obtain blood samples for laboratory testing in hospitalized pediatric patients.1 Accordingly, venous access is frequently practiced at every pediatric hospital.2,3 Vascular access includes peripheral intravenous catheters (PIVs), central venous catheters, and peripherally inserted central catheters (PICCs). Of these 3 options, PIV access is the simplest, least invasive, least expensive, and most commonly used method for short-term intravenous therapy needs.4
PIVs are nearly ubiquitous medical devices employed in caring for hospitalized pediatric patients.5 These are typically placed in the lower arm (hand or antecubital veins), although placement in upper arm veins and saphenous veins of the leg is also common. Other locations may be used as required by the patient's size and venous availability. In routine clinical practice, PIVs are used for short-term needs because studies have shown that rates of thrombophlebitis and device failure increase with longer dwell times.6 Although the average duration of pediatric hospitalization is approximately 96 hours, a recent study of 458 hospitalized pediatric patients showed the median PIV dwell time was only 29 hours, suggesting that multiple PIVs may be needed during a single admission.5,7 A study of PIVs placed in a pediatric emergency department showed that approximately 25% of these PIVs failed due to infiltration, dislodgement, phlebitis, or other causes, and nearly half of these required replacement.5 Another study of children presenting for anesthesia and surgery showed that approximately one third of PIVs were dysfunctional based on pain with palpation at insertion site, difficulty with injection of saline, infiltration at insertion site, or poor to no flow.8 Studies have also shown that PIV-associated complications, including malposition, infiltration, and extravasation, are more common in PIVs placed in children than in those placed in adult patients.9,10,11,12,13
Whereas high PIV failure rates are widely known and broadly accepted in pediatrics, the underlying reasons for failure are not well understood. We hypothesized that PIV failure is related to physical changes in the accessed vein associated with PIV catheter placement that cannot be appreciated during physical examination. Ultrasound (US) imaging, typically reserved for PIV catheter placement in patients with more challenging anatomy, enables greater vascular visualization.14 In addition, the American Institute of Ultrasound in Medicine has published practitioner guidelines for the use of US to identify peripheral venous complications.15 Therefore, an US imaging study was undertaken to evaluate and document venous morphology and flow in PIV-containing veins in hospitalized children. We also documented patient demographics, dwell time, and catheter gauge to identify any potential correlations.
Methods
Study design
This Institutional Review Board-approved, prospective pilot study was conducted at a large pediatric tertiary care center. A total of 35 patients between the ages of 3 and 15 years were enrolled. All patients had an existing PIV and were referred for PICC placement by the interventional radiology team. Patients requiring general anesthesia for PICC placement were excluded because any additional time required for the US study could potentially create unnecessary risk from prolonged anesthesia. Data from the first 5 patients were excluded from data analysis due to a learning curve in ensuring that high-quality US scanning and image capture was performed consistently. Data from the remaining 30 patients were used for final analysis. The interventional radiologists placing the PICC also assessed the US images to determine venous characteristics and anatomical changes. All patients were enrolled following a description of the study and verbal consent from the patient and caregiver. Patient demographics, including age, gender, weight, height, body mass index (BMI), and dominant hand were recorded. Using the electronic medical record, PIV information including dwell time, catheter gauge, location, and history of infusions was documented.
This is a descriptive study with primary outcomes to describe and document location of branches or collateral vessels, vessel diameter, and valve frequencies in pediatric veins with indwelling catheters. The secondary outcome is to describe how these venous properties and venous changes can be associated with indwelling PIV placement in order to improve PIV dwell time and reduce complications.
Procedure
An EPIQ 7 US unit with a L15-7io hockey stick transducer (Philips Ultrasound, Bothell, WA) was used for this study. Patients were placed in supine position with arm extended and the PIV-containing vein was scanned for a length of 10 cm centrally from the PIV insertion site. Ultrasound was used to measure and document venous diameter and depth from skin surface as well as location and number of venous valves and branches seen within the scanned segment. Morphological changes in vein lumen such as vein flattening or collapse and wall thickening were also documented. In addition, presence or absence of thrombus and blood flow around the catheter tip was evaluated. To calculate the percentage of vein lumen occluded by the PIV catheter, the known outer diameter of the 22- or 24-gauge PIV catheter was divided by the vein diameter as measured by US. The predicted venous flow was calculated by incorporating these diameters into Poiseuille's law. Color Doppler US imaging was used to better assess presence or absence of blood flow around the catheter and in the PIV-containing vein. If the accessed vein lumen was collapsed, saline flush was performed under US to determine if the collapse was fixed or reversible. Dynamic loop recordings were taken during and immediately after the flush.
Figure 1 shows a representative example of how the study was performed. A 10 cm segment of the accessed vein central to the PIV insertion site was scanned with US. The locations of valves and branch points were identified, marked, and evaluated for their distance from the PIV.
Statistical analysis
GraphPad Prism (GraphPad Inc, San Diego, CA) was used to perform all statistical analysis. Normality of data was deter mined using the D'Agostino-Pearson Omnibus Test. The mean, standard error (SE) of the mean, and the range of parameter values were reported.
Results
Patient characteristics
Data from 30 patients were analyzed. Patients were referred for PICC placement for a variety of reasons. Most commonly a PICC placement in this study was requested by the referring physician for long-term antibiotics for osteomyelitis, meningitis, cystic fibrosis exacerbation, or other infectious pathologies. Other indications included infusions for developmental delay and metabolic disorders. All patients were referred for PICC placement by physicians covering the inpatient hospital floor. The PIV used for the study was placed by a nurse or phlebotomist in the emergency room or on the floor. These patients were representative of a hospitalized pediatric population presenting for PICC placement by an interventional radiology team. There were 12 males and 18 females with a mean age of 11.7 years. The mean BMI was 19.3 kg/m2 (Table 1).
| Demographics | Mean ± SE (range) |
|---|---|
| Gender | 12 M/18 F |
| Age (years) | 11.7 ± 0.5 (5–15) |
| Body mass index (kg/m2) | 19.3 ± 0.6 (14–26) |
PIV characteristics
PIVs were located in the dominant extremity in 10 patients and the nondominant extremity in 20 patients; 22-gauge catheters were used in 15 patients and 24-gauge catheters were used in the remaining 15 patients. The mean PIV dwell time at time of US study (time since insertion) was 3.3 days. All PIV insertion sites were visibly normal with no physical signs of phlebitis (Table 2).
| PIV characteristics | Mean ± SE (range) |
|---|---|
| Dwell time (days) | 3.3 ± 0.5 (1–12) |
| Depth from skin surface (mm) | 2.07 ± 0.13 (0.89–3.64) |
| Diameter (mm) | 2.02 ± 0.18 (1.04–5.34) |
| Diameter of veins with 22-gauge PIV (mm) | 2.2 ± 0.3 (1.07–5.34) |
| Diameter of veins with 24-gauge PIV (mm) | 1.9 ± 0.2 (1.04–3.69) |
| Number of 22-gauge PIVs/number of 24-gauge PIVs | 15/15 |
| Laterality of PIV (dominant/nondominant) | 10/20 |
PIV=peripheral intravenous catheter
Venous characteristics and PIV-associated findings seen with ultrasound
The mean depth of accessed veins from the skin surface was 2.07 mm. The mean diameter of the accessed veins was 2.02 mm. The mean diameter of veins containing a 22-gauge catheter was 2.2 mm, and the mean diameter of veins containing a 24-gauge catheter was 1.9 mm. Hospital PIV policy suggests that a 24-gauge catheter be placed in all children younger than 3 years of age and that a 22-gauge catheter be used in children older than 3 years. Whereas 22-gauge PIVs were used consistently in the larger veins, the choice of PIV gauge in veins 1 to 2 mm in diameter was inconsistent. Using vein diameter measurements obtained from US scans and the known diameter of each catheter, the mean vein occlusion among all 30 patients was 50%.
Ultrasound showed at least 1 branch point in 22 out of 30 (73%) and 2 branch points in 15 out of 30 (50%) scanned venous segments. Twelve out of 30 veins (40%) had at least 1 valve and 3 out of 30 veins (10%) had 2 valves. No venous valves were identified with US in the remaining 60%. Figure 2 shows representative US images of venous branches, and Figure 3 shows representative images of valves seen on US images. Presence of a valve did not always correlate with the location of a branch. Additionally, presence and number of valves did not correlate with location within the arm (ie proximal or distal or upper arm versus forearm).
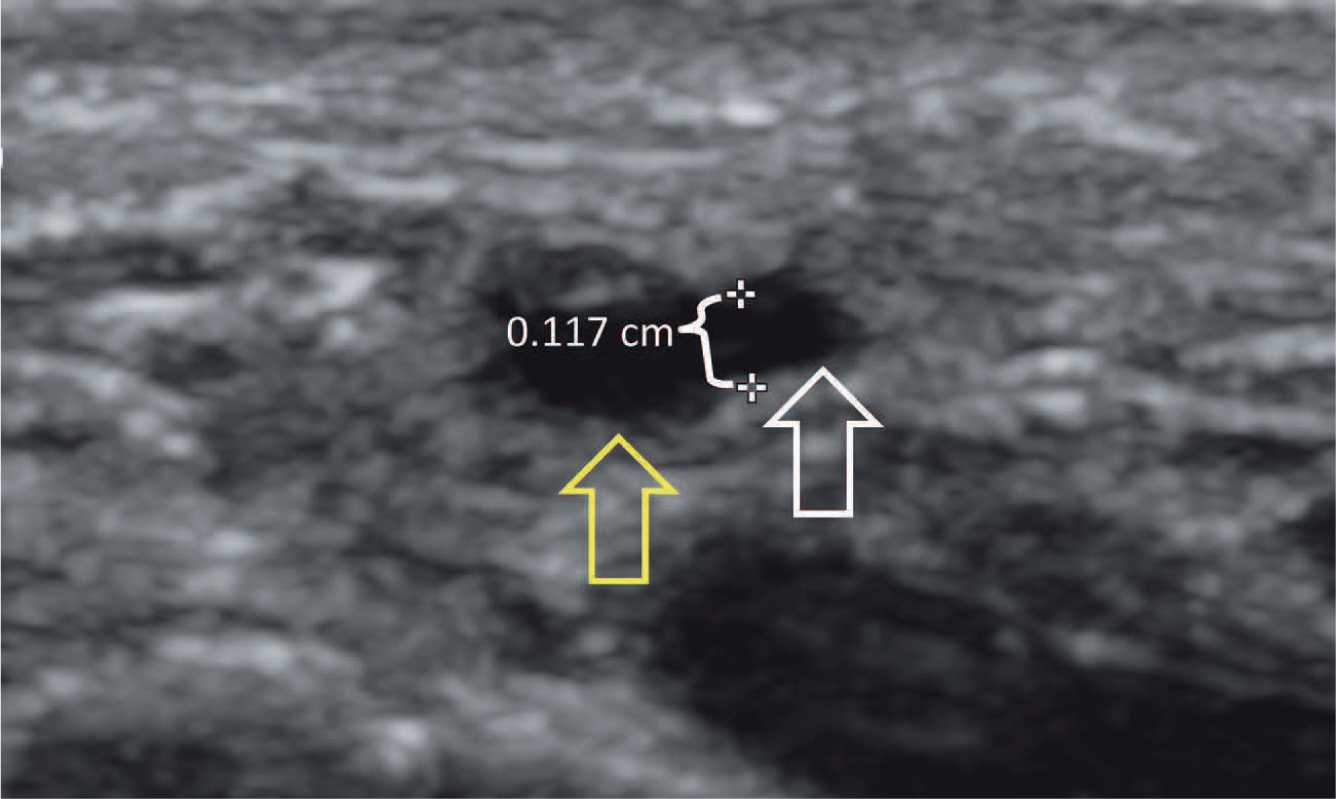

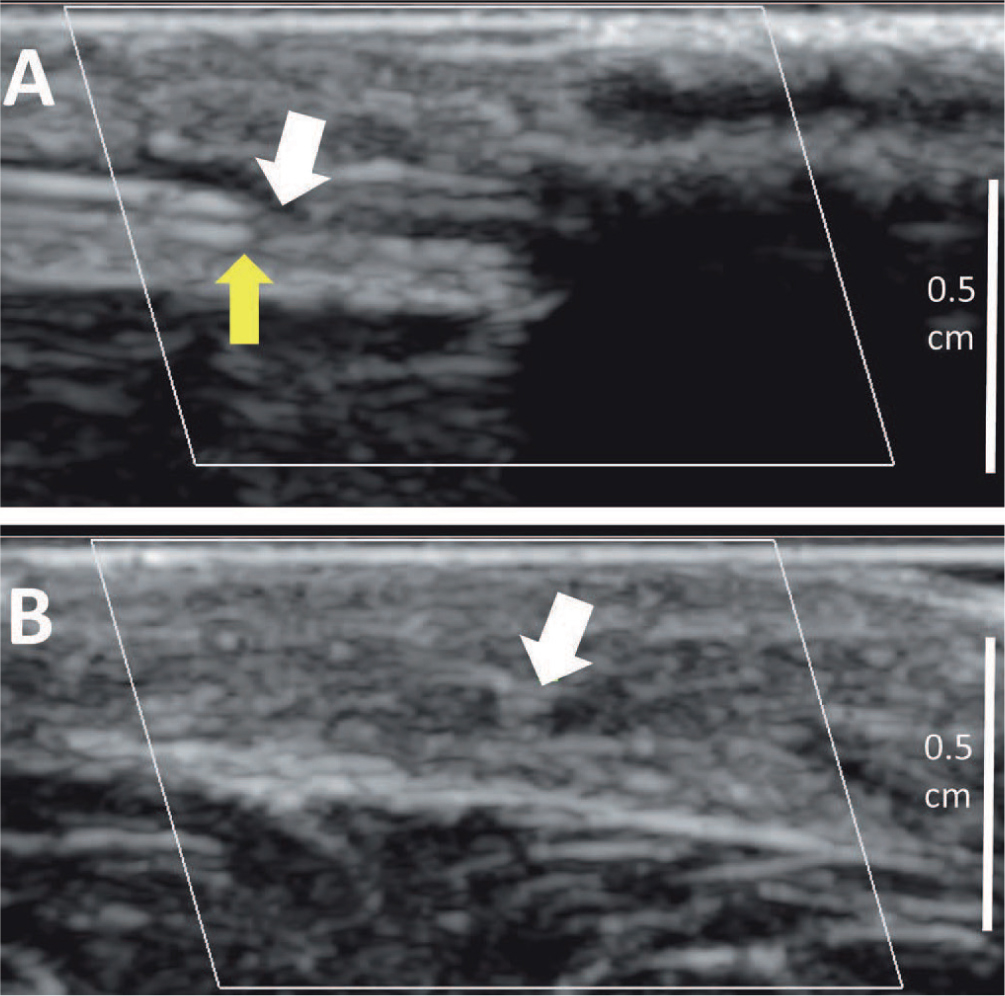
The 3 most common venous findings associated with indwelling PIVs included luminal narrowing, wall thickening, and presence of thrombus. Luminal narrowing is marked or complete collapse of the vein proximal (closer to the heart) to the catheter tip is marked and limits further tracing of the vein course, as shown in Figures 4A and 4B. Wall thickening is seen as a circumferential prominence of the vein wall but with a persistent, patent, and compressible lumen as shown in Figure 5. Thrombus is seen as a noncompressible echogenic material inside the vein lumen as shown in Figures 6A and 6B.
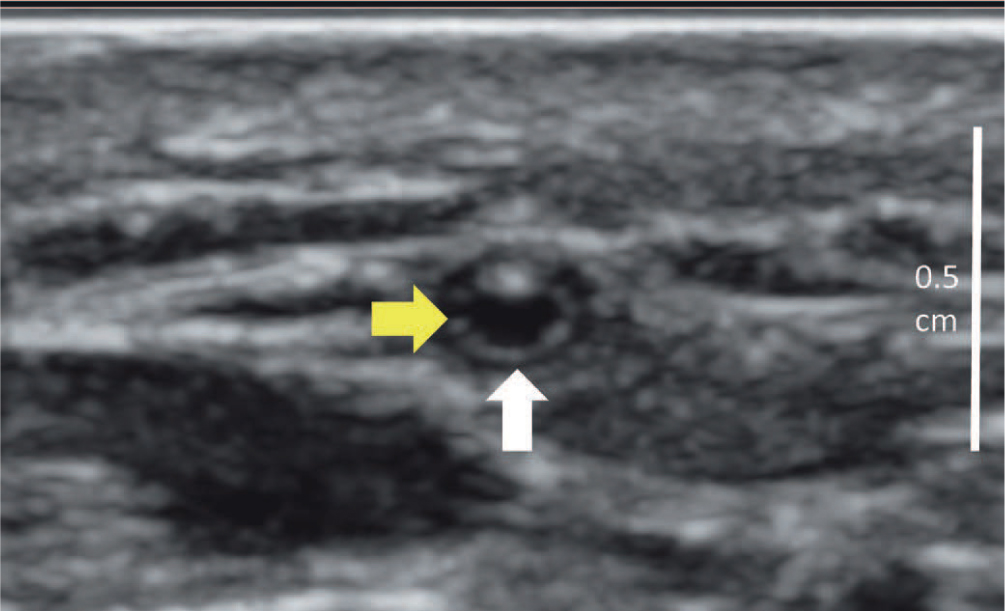

Fourteen of the 30 veins (47%) showed marked narrowing of their lumen central to the PIV catheter tip. Ten out of 30 veins (33%) showed wall thickening central to the PIV, and 6 of the 30 veins (20%) contained some degree of PIV-associated thrombus. Ultrasound imaging confirmed that the thrombus was occlusive in 3 veins and nonocclusive in the other 3 veins (Table 3).
| Ultrasound venous findings | Fraction (%) of patients |
|---|---|
| Presence of flow at PIV tip | 18/30 (60) |
| Presence of flow at 10 cm mark | 21/30 (70) |
| Thrombus at PIV tip | 6/30 (20) |
| Venous wall thickening | 10/30 (33) |
| Collapse/spasm at PIV tip | 14/30 (47) |
| At least 1 branch | 22/30 (73) |
| At least 1 valve | 12/30 (40) |
PIV=peripheral intravenous catheter
To better understand the nature of venous narrowing and collapse, these veins were flushed with normal saline under US. The video loop demonstrates temporary restoration of the vein lumen and patency during saline flush (Supplementary Movie S1).
A notable finding was that the veins that were collapsed adjacent to the PIV tip with absent flow but had a branch point distal to the PIV tip showed a restored lumen and blood flow following the branch point all the way to the 10 cm mark. Figure 7 shows an example of a vein segment with absent flow at PIV tip but detectable flow on color Doppler following a branch point. Lastly, 8 of the 30 scanned vein segments had minimal to no notable venous morphology changes visible with US. These veins were normal in appearance, were patent with consistent detectable flow, and had no detectable changes with US imaging.

Discussion
The purpose of this study was to identify, document, and describe venous changes associated with PIV placement using US imaging in order to better understand factors that may contribute to high rates of PIV failure in children. Venous changes including narrowing, wall thickening, and presence of thrombus at the PIV tip were noted in 22 (76%) of the evaluated veins, even in the absence of any clinical signs and symptoms. These changes can reduce blood flow around the PIV and within the accessed vein, potentially contributing to early device failure and inability to aspirate blood through the PIV.
Fourteen veins (47%) showed venous narrowing central to the PIV tip. This venous narrowing may be related to a reduction in the blood flow needed to keep the vein fully distended and patent in the presence of the PIV. An analysis of the venous diameter relative to the catheter diameter showed that when the catheter occupied <40% of the vein diameter, the accessed veins were more likely to have identifiable blood flow with color Doppler imaging. At the same time, these veins were also less likely to show venous narrowing. It was expected that flushing the PIV with saline would help restore the narrowed or collapsed vein lumen and subsequently keep it patent. Yet, in all cases, the vein lumen could be expanded during the saline flush but returned to the narrowed or collapsed state after flushing was completed.
Ten veins (33%) had venous wall thickening central to the PIV tip. It has been suspected that movement of the PIV inside the vein may create mechanical irritation of the venous endothelium and vein wall. However, in many cases, the wall thickening was noted distal to the PIV tip, suggesting that it might be created by chemical irritation of vesicant infusions or potentially other factors. Helm et al.6 suggest that PIV properties including gauge, length, stiffness, and composition material may constitute mechanical phlebitis from traumatic movement of the catheter within the vessel lumen. An additional factor for mechanical irritation is body movement relative to the catheter.6 The thickening of the vein intima was not reversible with saline flush. Although the evaluated veins did not show external signs of phlebitis, the internal venous changes seen with US may be predictive of future phlebitis or thrombophlebitis.
Six veins (20%) had venous thrombus. This was unexpected because the studied PIVs were presumably maintained according to hospital PIV policy, which recommends that saline flushes be performed at every nurse shift change and as needed to determine or maintain PIV patency. Additionally, the observed thrombi were not reduced after saline flush, suggesting that the presence and accumulation of thrombus may lead to PIV malfunction over time.
Observing the saline flush using US imaging also provided insights into one possible cause of PIV-related complications. Temporary restoration of vein lumen and patency seen with US during saline flush implies that the collapse of the vein is reversible and may be a gradual process potentially triggered by blood flow reduction. Collapse of veins adjacent to the PIV tip but distally restored lumen and flow suggest that the collapse was due to a reduction or loss of blood flow and can be reversed or prevented by maintaining blood flow around the PIV tip.
Although PIV access plays an important role in management of hospitalized pediatric patients, it can be an anxiety-inducing and painful procedure for children. Venipuncture and intravenous catheterization have been reported to be the two most common sources of pain in hospitalized children.16 At the same time, pediatric veins are only a few millimeters in diameter and securing safe access can be technically difficult for the care provider.17 In addition, PIV replacement is also associated with increased cost. It is estimated that the cost of a first-time successful PIV placement is between $28 and $35 but increases when failed catheters are identified and have to be replaced.6 One study showed that the cost of PIV placement including nursing costs, supply costs, multiple attempts, and replacement can exceed $113,000 per year in a 30-bed pediatric hospital.18 Therefore, solutions that address early device failure and prolong PIV dwell time could reduce pain and anxiety for children and reduce cost for pediatric hospitals.
This study was designed to describe PIV-associated venous changes using US imaging. Although these changes were correlated with patient demographics and PIV properties that may lead to PIV device failure, a limitation of the study was that it did not fully address other factors that contribute to PIV device failure. For example, the type of medications infused through the PIV and relevant past medical history were not extensively evaluated in this study. A further limitation is the difficulty of US imaging to visualize pediatric anatomy. Despite the use of a high-resolution transducer and a high-end diagnostic US unit, valves in pediatric patients may be difficult to visualize due to their small size and may be underreported. In addition, the limited sample size and restriction in age range of this initial pilot study provide limited generalizability to the entire pediatric population but merit further analysis through a larger study.
Conclusion
The overall results of this study demonstrate that subclinical venous changes are present and detectable with US in nearly 3 out of 4 accessed veins after PIV placement in children. Changes such as luminal narrowing, wall thickening, and presence of thrombus can reduce blood flow around the PIV tip and may lead to PIV failure, resulting in the inability to aspirate blood from PIVs. Only 26% of the evaluated veins showed normal caliber and flow throughout the 10-cm scanned segment. Perhaps most notable was that none of the patients showed any external signs of phlebitis or vein irritation, although 2 patients reported pain during flushing of the PIV. These interesting findings are based on a small sample cohort of 30 pediatric patients, and a larger study is needed to further understand the causes of PIV malfunction and failure in children.