

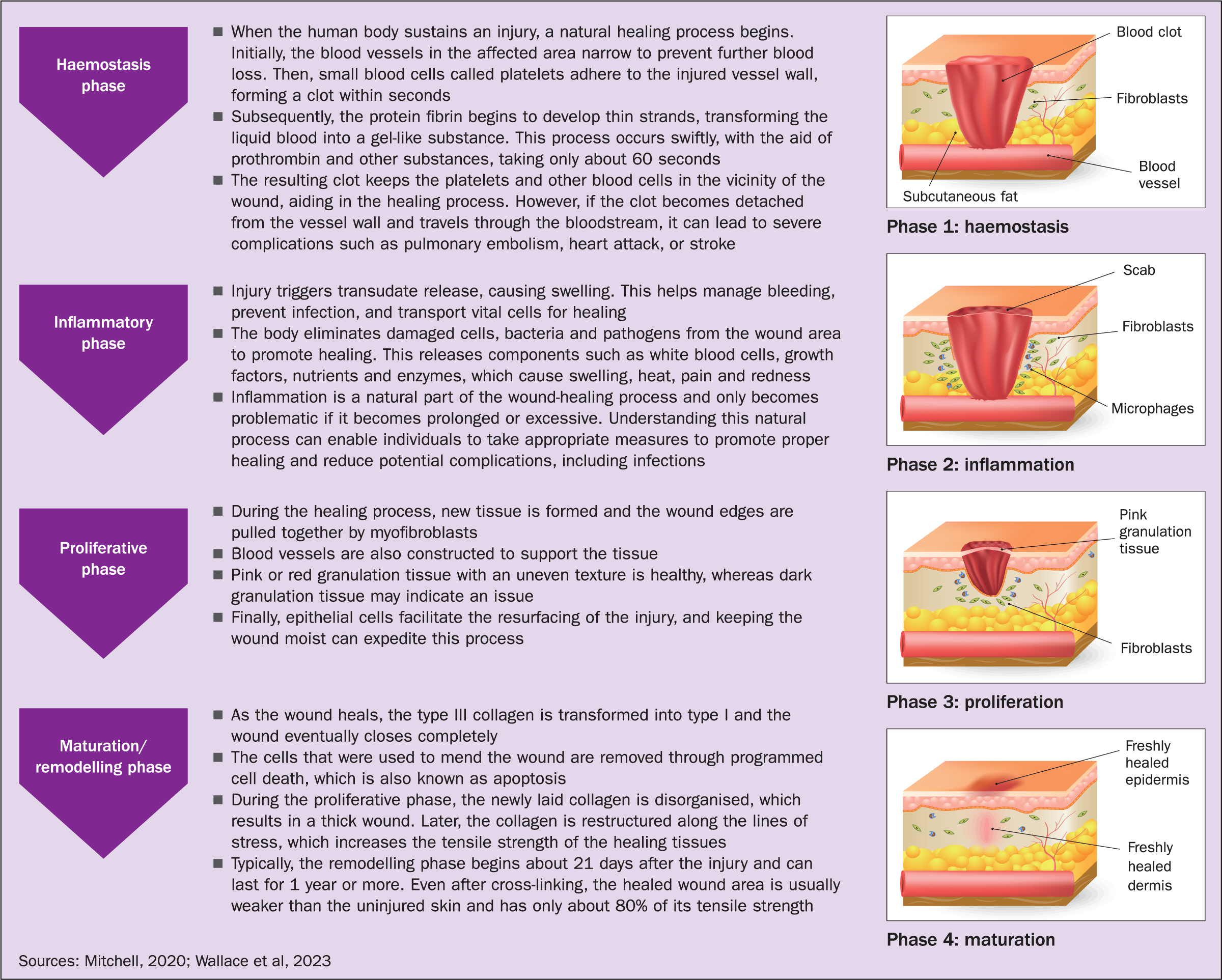
Wound healing is the process by which the body replaces and restores damaged tissue (Greaves et al, 2013) and enhanced mechanisms such as regeneration and tissue repair are initiated to help the healing process. It is a normal biological process that follows precisely programmed and highly regulated phases (Wallace et al, 2023). Wound healing is generally described as having four distinct phases: homeostasis, the defensive and inflammatory phase, the proliferative phase, and finally the maturation phase (Peate and Stephens, 2020). These phases are collectively referred to as the healing cascade and work together to promote the healing of wounds (Figure 1). For a wound to heal effectively all four phases must occur in the proper sequence and time frame (Coloplast, 2023). However, as the healing process involves a complex interaction of physical, chemical and cellular events, a multitude of factors can interfere with one or more phases of the process, leading to improper or impaired wound healing.
Tissue regeneration
The body is capable of regenerating certain types of cells, such as epithelial cells and this is considered the most effective method of healing, as the regenerated tissue retains the same functionality and appearance.
Tissue repair
This is a complex process that can result in visible alterations to the repaired area as the body repairs damaged or destroyed dermal or subcutaneous tissue. Consequently, during this process, the repaired tissue loses its specialised function and original structure, leading to scarring and changes in the skin's appearance.
Healing by primary, secondary and tertiary intention
It is identified that there are three ways that wounds heal: primary intention, secondary intention and tertiary intention, depending on the wound type and the cause of the injury. Mitchell (2020) suggested that the healing process is essentially the same, although the timescales may differ.
Primary intention
Surgical incisions with minimal tissue loss can heal quickly through primary intention healing, and can be closed using sutures, staples or clips (Curr and Fordham-Clarke, 2022). This healing is uncomplicated, with minimal scarring and no tissue deficit; however, the time to heal depends on overall health status, with the initial union of wound edges taking 7-10 days and the maturation stage taking up to 2 years.
Secondary intention
When there is significant tissue loss, wounds heal through a process called secondary intention, which involves the wound being left open and left to heal by contraction, granulation, and epithelialisation (Peate and Stephens, 2020). The body produces granulation tissue to fill in the tissue deficit before forming scar tissue, and the healing timeframe is usually significantly longer than healing by primary intention.
Tertiary/third or delayed intention
This involves intentionally keeping a wound open to allow for swelling or infection to resolve. It is a form of healing by delayed primary intention, which leaves more scarring than when a wound is left to heal by primary intention, but the timeframe will be shorter than when a wound heals by secondary intention (Mitchell and Llumigusin, 2021).
Granulation tissue
Granulation tissue is often characterised as red, bumpy tissue (Figure 2a), and may be described as ‘cobblestone-like’ in appearance (Naughton, 2021). It contains new blood vessels and collagen, and is often moist. Care must be taken when coming into contact with it because it is highly vascular and can bleed easily with minimal trauma (Peate and Stephens, 2020).
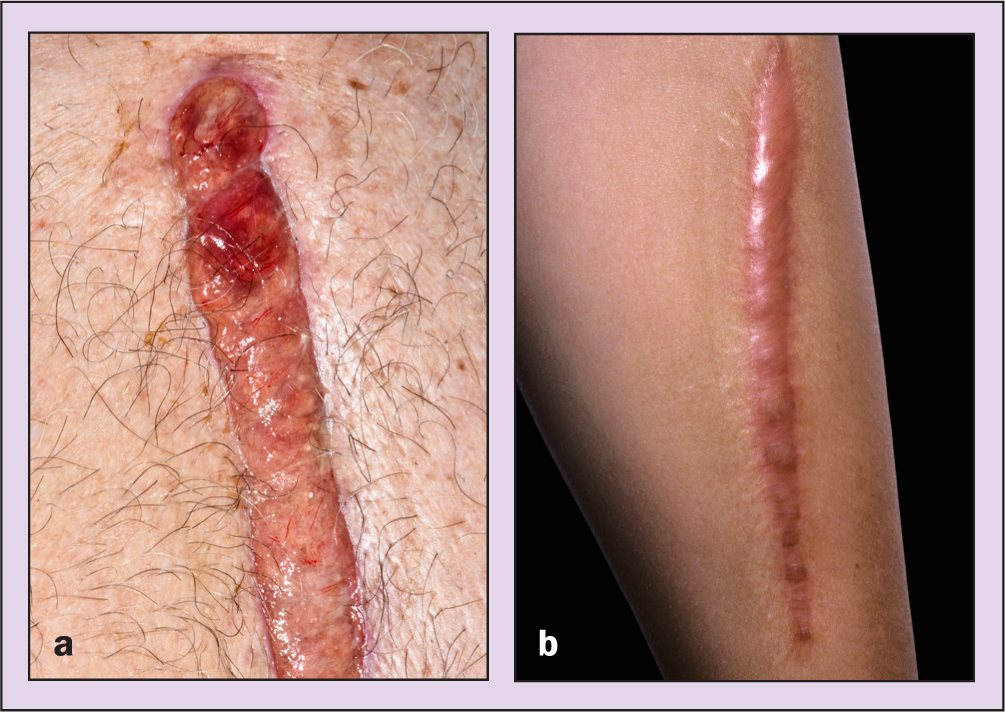
Not all wounds heal evenly, which will depend on a number of factors, as outlined below. For example, hypotrophic granulation tissue typically exhibits specific characteristics. It appears smooth, pink, or even slightly pale in colour. This appearance can be indicative of inadequate perfusion or blood supply to the affected area. Several factors can contribute to the development of hypotrophic granulation tissue, including pressure, trauma or infection.
Hypertrophic granulation, also known as hypergranulation, is frequently an indicator of excessive moisture or the possibility of infection. It is characterised by its moist and red appearance and tends to extend beyond the surface of the wound (Figure 2b).
This overgrowth can impede the process of epithelialisation, the formation of new surface skin, and heightens the risk of developing scars (Mitchell and Llumigusin, 2021).
What are staples?
Surgical staples, also known simply as staples or clips, are medical devices used to close wounds and incisions created during surgical procedures or in the event of injuries (Thomas, 2015). As an alternative to traditional sutures, they are typically made of stainless steel or titanium and come in various sizes and shapes, depending on the specific surgical application. They are a crucial part of wound management and play a significant role in facilitating the natural healing process of tissues for wounds closed via primary intention. They enable the edges of a wound or incision to be brought together, allowing for proper alignment of tissue layers, and reducing the risk of foreign materials and bacteria entering the body. They assist in holding the tissue in place, which supports the body's natural healing mechanisms provides stability and reduces tension on the wound, leading to scar formation.
Starting in the late 1990s, surgical staples garnered significant interest as effective tools for closing wounds due to their numerous advantages compared with traditional sutures. These benefits have led to their widespread adoption, particularly in certain surgical fields. They are often quicker and simpler to use, which is beneficial for surgeries involving large incisions and in emergencies when time is critical. It has also been suggested that they cause less tissue damage, promote faster healing, and if applied correctly and managed appropriately can reduce the risk of infection (Ghosh et al, 2022).
From an application perspective, their use reduces the risk of needlestick injuries, and they also provide uniform tension across the wound, resulting in a more consistent closure, whereas sutures may be subject to variations in tension applied by the surgeon. However, staples can often be more expensive if incorrectly placed, and can lead to wound healing complications; they are also inappropriate for delicate tissues or areas with high tension. Due to their construction, staples are not absorbable and therefore need to be removed post surgery. Some individuals may also develop allergic reactions to having them in situ.
Surgical site infections
Surgical site infections (SSIs) are the third most commonly reported type of healthcare-associated infection and the most costly, posing significant risks to patients, families and healthcare systems (World Health Organization (WHO), 2018; Hegarty et al, 2019; Stryja et al, 2020). These infections can escalate into life-threatening conditions, increasing patient morbidity and mortality (WHO, 2018). Many SSIs may go unreported, distorting data on their true impact (Oliveira et al, 2007).
Furthermore, there is a lack of standardised education for clinicians on dressing surgical wounds. Research by Horgan et al (2023) demonstrated that health professionals' knowledge and attitudes towards SSIs and surveillance are poor. However, attitudes were generally positive, particularly concerning the health professional's role in prevention.
Aseptic non-touch technique
The aseptic non-touch technique (ANTT) is a method employed to minimise the likelihood of patients contracting infections during clinical procedures. It accomplishes this by safeguarding ‘key parts’ and ‘key sites’ from microorganisms that might be transmitted from healthcare personnel or nearby environments. Key sites are classified as parts of the body into which infection might be introduced during a procedure, eg an opening in the skin, the urethra or a cannula insertion site, whereas key parts are associated with the equipment that might come into contact with key sites or other key parts, eg dressings, catheters and syringe tips. These should not be touched or touched only with sterile gloves and sterile equipment.
There are two main variations of ANTT:
- Standard approach, which is used for uncomplicated, simple and quick procedures involving few key sites or key parts
- Surgical approach, for those skills and procedures that are more complex, lengthy and involve a large number of/or multiple key sites or key parts.
When carrying out a clinical procedure, an ANTT risk assessment is required to ascertain whether the procedure necessitates the adoption of a standard or surgical ANTT approach. This involves assessing the difficulty of protecting the key parts and sites associated with the skill, while considering the number and sizes of the key parts, environment, invasiveness, and user competency (Mitchell, 2022).
For standard ANTT procedures, non-sterile gloves can be worn because the key parts and key sites are limited, for example when undertaking cannulation and venepuncture. However, for surgical ANTT procedures, such as urinary catheterisation and wound care, sterile gloves must be worn, due to the level of invasiveness (Mitchell, 2022).
Informed consent, patient preparation and pain management
Where possible, informed patient consent should be obtained. This will include ensuring that patients are aware of the reasons for the removal of the staples, the associated risks and complications, and details of the removal procedure and aftercare (Lister et al, 2021). Providing this level of information will not only safeguard that the patient can provide valid consent, but it will also assist in building rapport and a trusting therapeutic relationship, which can help reduce any fears or anxieties a patient may have. The timing of staple removal depends on various factors, including the surgeon's instructions, the comorbidities of the patient and the specific area of the body where the staples are located (areas with increased vascularity can usually be removed more quickly than the standard timeframe of 7-10 days (Curr and Fordham-Clarke, 2022).
It is also important to consider not only the patient's comfort, but also the potential to increase their pain. Thus appropriate multimodal approaches to pain assessment and management need to be taken in order to minimise the risks of patient harm. This can include the use of pharmacological and non-pharmacological approaches, such as distraction therapy and non-opioid analgesics (Ford, 2019).
How to remove staples
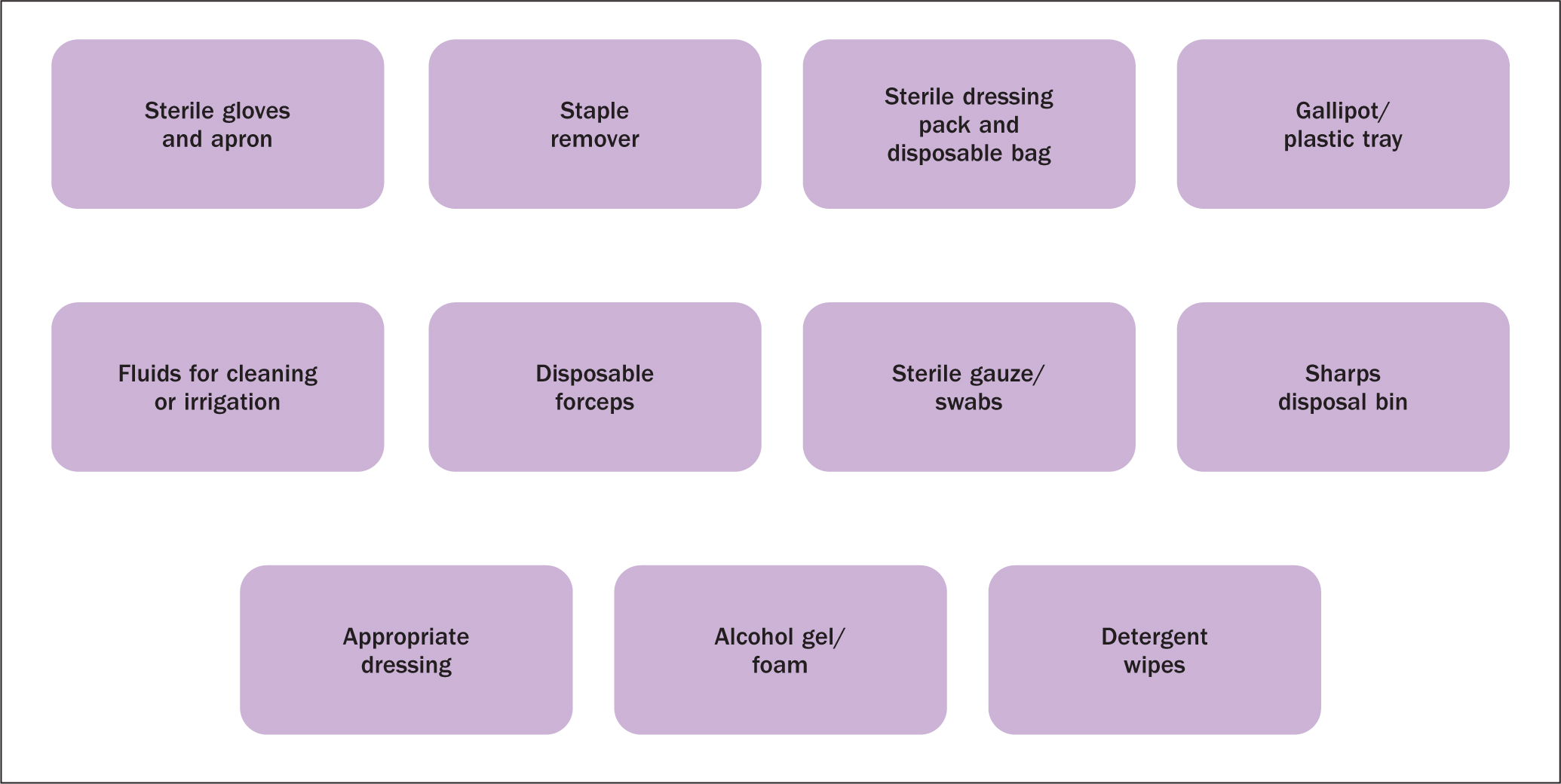
To carry out the procedure, specific equipment is required (Figure 3), all of which should be checked before carrying out before proceeding with staple removal:
- Before carrying out a clinical skill, you must communicate with your patient and provide them with the relevant information to gain informed consent. This will also provide you with the opportunity to talk about previous experiences of suture removal, ascertain whether the patient has any allergies to dressings, assess for potential complications and physically prepare the patient and the environment before assembling the equipment
- Decontaminate your hands using the appropriate hand-washing technique
- Next, you must ensure that the surfaces you are using are cleaned in line with local policy
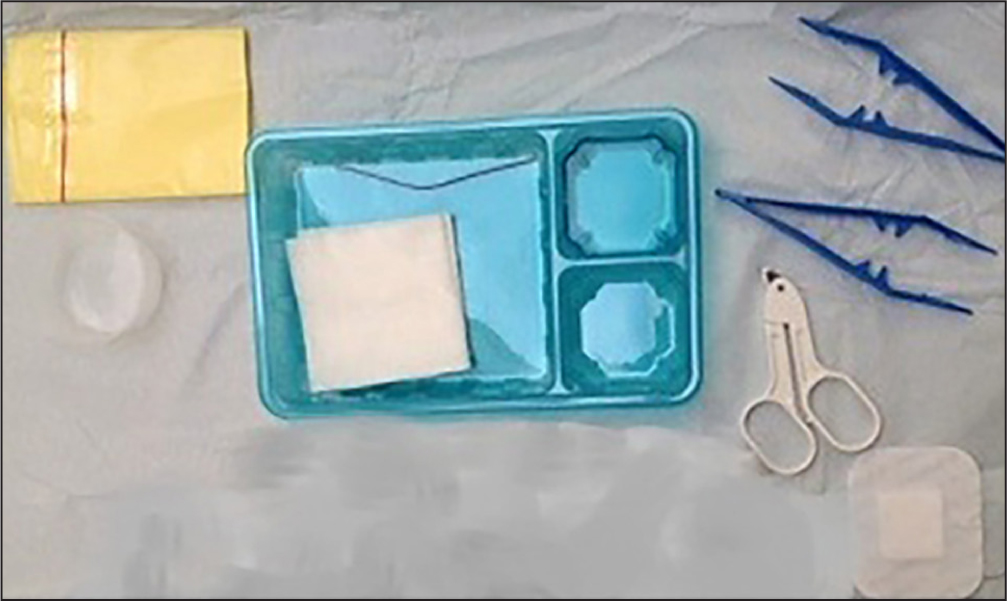
- When gathering the required equipment, take the opportunity to examine the expiry date of the items, as well as the external packaging for perforations, tears, decolourisation, moisture and other signs of possible contamination (Figure 4)
- Disposable single-use plastic aprons must be worn when carrying out the clinical procedure. These may be colour-coded, often used for specific tasks, and the colours may differ depending on individual trust practices. Torn or otherwise damaged aprons must not be used
- Remove the sterile dressing pack from its outer packaging, and place it on a clean, dry, flat work surface. Using your fingertips and touching the outer surface of the paper only, open the pack and lay it flat to create a sterile field
- Taking care not to contaminate the sterile field carefully open the dressing and other equipment required onto the opened dressing pack (Figure 5)
- Reapply alcohol hand gel and allow to dry before donning the sterile gloves
- Once the gloves have been donned, you may commence the procedure
- Before removing any staples, a full assessment of the wound must be undertaken, to judge whether to remove all of the staples (Figure 6a). If any sign of wound separation is visible it may be possible to remove alternative staples, with the view to removing more at a later stage
- Assessment of the wound will include skin integrity, uniform closure of the wound line, condition of the wound edges, colour, exudate, signs of inflammation and odour. If there are obvious signs of infection, follow local policy
- If needed, clean the wound with 0.9% sodium chloride to remove dried exudate and blood
- Explain to the patient that they may feel tugging and pulling, but the procedure should not be painful
- Hold the staple remover in your non-dominant hand and slide the bar closest to the skin under the staple. The V-shaped groove should be under the clip at an angle of 90° (Figure 6b)
- Bring the handles of the staple remover together and this action will move the bars that grasp the staple, bending it in the middle and as a counteraction force to raise the ends of the staples out of the skin (Figure 6c)
- If the wound in under tension, use the non-dominant hand to assist with the staple removal and support the surrounding tissue
- Place the removed staple in a gallipot or dressing gauze (Figure 6d), depending on the available equipment. When you have completed removal of staples, this will allow you to confirm the number of staples you have removed matches the number of staples that were inserted
- Repeat the above process, remembering to remove alternative staples (if appropriate) and continually observe the wound response. Once all the staples are removed, check the patient's comfort and dress the wound appropriately (Figure 6e)
- Dispose of waste, remove your personal protective equipment (PPE) and decontaminate hands using the appropriate technique (Ford and Park, 2018; 2019)
- Document your care (via paper-based or electronic platforms) according to trust guidelines and protocols. This should include, as a minimum standard, your signature, date and designation, the time, how many staples were removed, the condition of the suture line and surrounding skin, signs of infection and any other post-surgical wound complications.


Conclusion
Staple removal is a clinical skill that necessitates a thorough understanding of its principles and techniques, and alignment with clinical procedures. To stay current in practice, it is crucial to regularly review local and national guidelines, engage in practical exercises, and incorporate alternative educational methods like simulation training.
KEY POINTS
- Nurses must employ aseptic non-touch technique to prevent infections during the removal of surgical staples. This method protects key parts and key sites from contamination, which is crucial for reducing the risk of post-surgical infections and promoting effective wound healing
- It is essential for nurses to have a thorough understanding of the different phases of wound healing – haemostasis, inflammation, proliferation, and maturation. Knowledge of these stages allows for better wound assessment, timely intervention and appropriate care, which are critical when managing surgical sites, especially those closed with staples
- Prior to staple removal, nurses should ensure that patients are adequately informed about the procedure to obtain informed consent. This includes discussing potential risks, the reasons for staple removal, and any post-procedure care. Effective communication helps build a trusting relationship with the patient and can alleviate anxiety related to the procedure