

Intravenous (IV) fluids are commonly prescribed in hospitals, with foundation doctors and nursing teams closely involved in fluid assessment, prescription, administration, and ongoing management (Ghosh and Maltez, 2019; Crowe, 2023). However, foundation doctors report a lack of preparedness around prescribing IV fluids and have limited experience in fluid assessment and management, and previous work regarding nurses has reported knowledge gaps in fluid balance assessment and monitoring (Powell et al, 2013; Wuyts et al, 2022; Crowe, 2023). This translates into an increased number of prescribing errors in clinical areas, such as the emergency department (ED) and general wards, compared with critical care units and operating theatres, where more experienced clinicians are located. It is worth noting that incorrect IV fluid prescription has been shown to cause significant morbidity and mortality, with 1 in 5 IV fluid recipients experiencing complications due to inappropriate fluid prescriptions (Callum et al, 1999).
At a large NHS trust in England, there were no data regarding the quality of assessment and management of patients requiring IV fluid, specifically regarding adherence to the National Institute for Health and Care Excellence (NICE) guideline CG174 (NICE), 2017a). The authors were involved in a project of work to examine this.
Aims
Method
Shared learning examples available on the NICE website regarding the guideline were reviewed to identify learning points for project design and scope adherence in other trusts (NICE, 2017b). Twelve audit standards were then developed and mapped to the guideline, consisting of four main algorithms: assessment, resuscitation, maintenance, and replacement/redistribution (Table 1). The 12 audit standards were tested using real patient data (pilot data, not included in final analysis) and an electronic data collection tool developed. A target adherence of 95% for each standard was set.
| 1 | The patient&s fluid and electrolyte needs are assessed prior to IV fluid prescription |
| 2 | The following information is included in the IV prescription:
|
| 3 | Patients receiving IV routine maintenance fluids* have an IV fluid management plan |
| 4 | The IV fluid management plan, for patients requiring >24 hours fluid administration, includes the following:
|
| 5 | For patients in need of fluid resuscitation:
|
| 6 | Patients who have received initial fluid resuscitation are reassessed using the ABCDE approach |
| 7 | Patients who have already been given >2000ml of crystalloids and still need fluid resuscitation after reassessment receive expert help |
| 8 | Patients who have not had >2000 ml of crystalloids and who still need fluid resuscitation after reassessment receive 250–500 ml of crystalloids and have a further reassessment using the ABCDE approach |
| 9 | Patients who are showing signs of shock but do not need fluid resuscitation after reassessment receive expert help |
| 10 | If patients need IV fluids for routine maintenance alone, the initial prescription is restricted to:
|
| 11 | IV fluid prescriptions are adjusted to ideal body weight in obese patients a. Expert help sought if BMI>40 |
| 12 | IV fluid prescriptions are adjusted to account for fluid/electrolyte deficits or abnormal distribution
|
Data were collected between September 2022 and May 2023 across 29 clinical areas of the NHS trust, with inclusion criteria being patients who had been prescribed and received IV fluids at any time during their inpatient episode. To minimise researcher bias and ensure consistent data collection, collaborators were trained using the electronic data tool on real patient cases prior to data collection, and one collaborator was present for every data collection session.
Results
Demographics
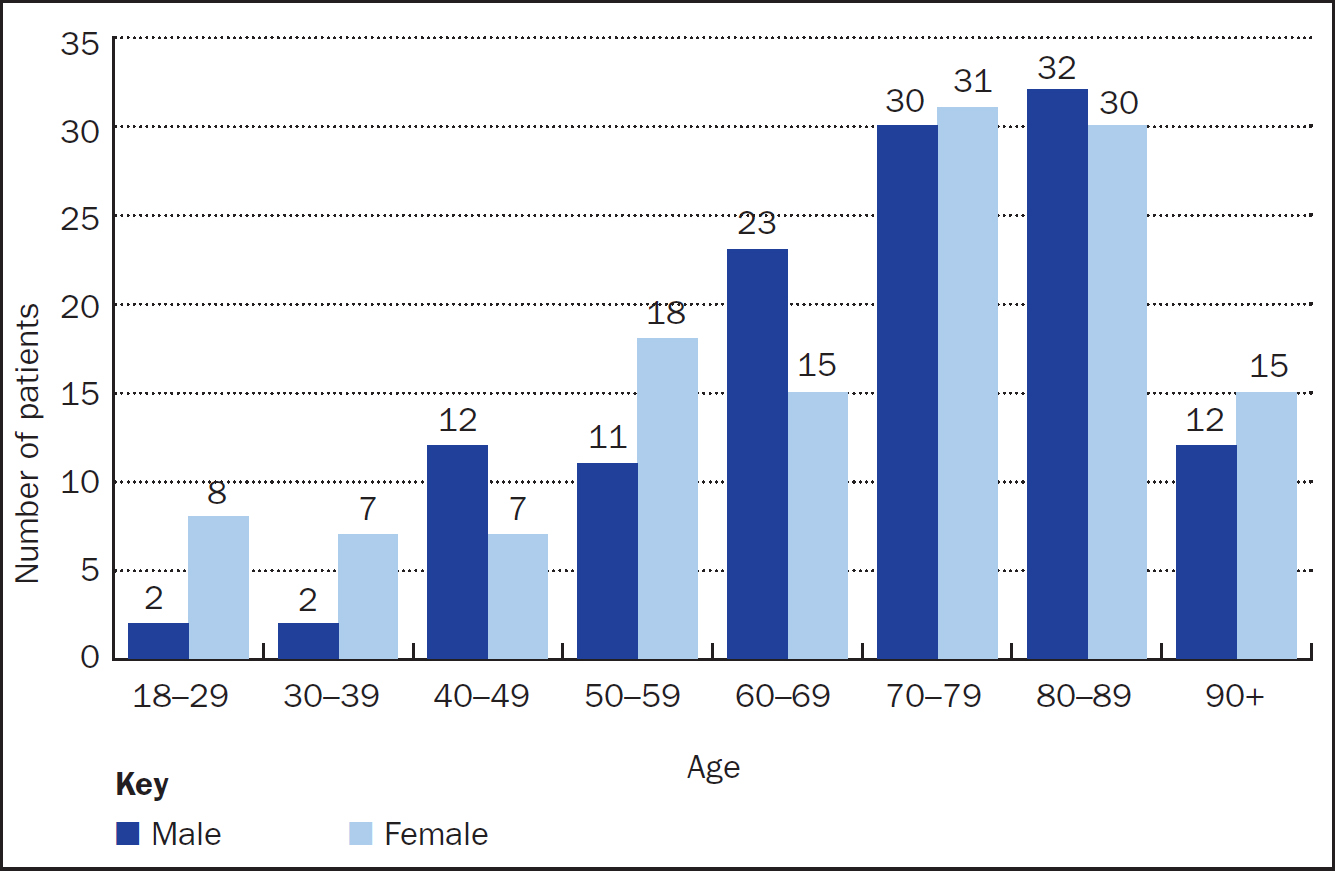
The number of patients satisfying the inclusion criteria was 255, totalling 335 separate IV fluid prescriptions. White British patients and patients in the 70–89 years age group formed most of the patient population (Table 2, Figure 1).
| Male | Female | |
|---|---|---|
| White British | 112 | 116 |
| Asian – Other | 0 | 1 |
| Black African or British Black African | 2 | 0 |
| Black Caribbean or British Black Caribbean | 1 | 2 |
| Indian or British Indian | 1 | 0 |
| Mixed White and Black African | 0 | 1 |
| Mixed White and Black Caribbean | 1 | 0 |
| Pakistani or British Pakistani | 2 | 2 |
| Any other Black Background | 1 | 3 |
| Any other ethnic group | 1 | 1 |
| Any other Mixed Background | 0 | 1 |
| Any other White Background | 1 | 2 |
| Unknown | 2 | 1 |
During hospital admission, 80 patients required a combination of IV fluid resuscitation and IV fluid maintenance, 22 patients required resuscitation fluids only, and 153 required routine maintenance fluids only.
Standard 1. Assessment of fluid and electrolyte requirements
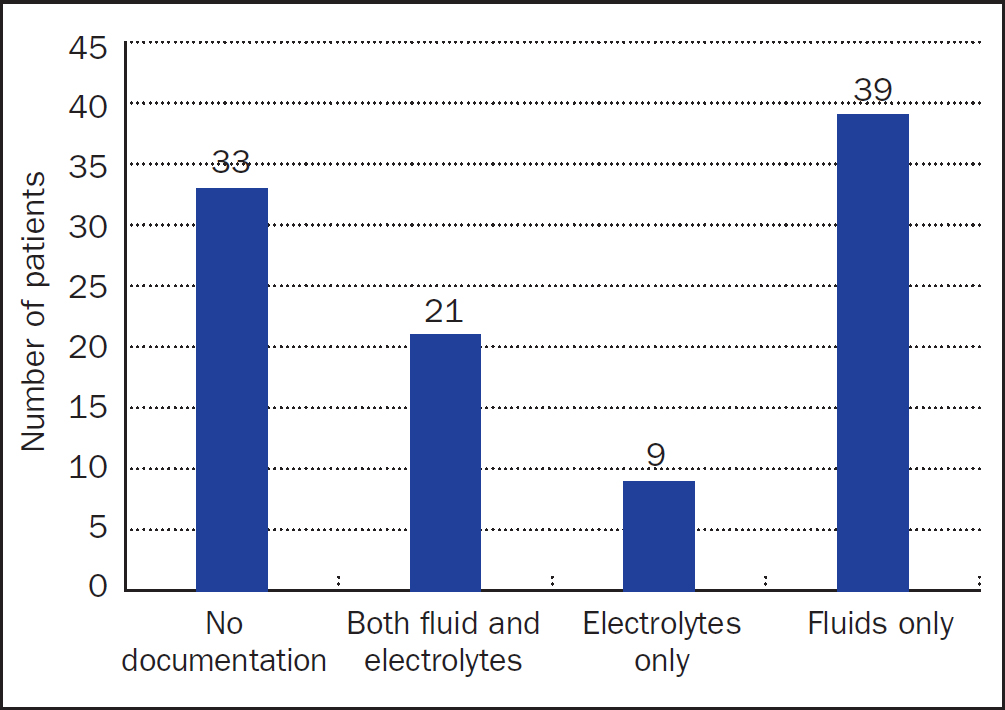
A documented ABCDE assessment at the time of initial IV fluid resuscitation prescription was made in 53/102 patients, a non-ABCDE assessment in 37/102 patients, and there was no documented evidence of assessment in 12/102 patients. No documentation of fluid status was made for 73/102 and was clearly documented in only 5 patients, with a reference to fluid status made in a further 24 patients. Regarding assessment of fluid and electrolyte needs, documentation of assessed fluid needs only or no documentation of fluid or electrolyte needs were most common (Figure 2).
Most patients (88/233) did not have documented fluid or electrolyte assessment at the time of initial IV fluid maintenance prescription and only 60 had an assessment of both fluid and electrolyte needs.
To support assessment of fluid and electrolyte needs, history, clinical examination, clinical monitoring, and laboratory assessments should be considered. All four of these factors were considered in 25/60 patients who had an assessment of both fluid and electrolyte needs.
In summary, there was a 21% adherence and 26% adherence to fluid and electrolyte needs assessment respectively, prior to IV fluid prescription, for patients receiving IV fluid resuscitation and IV fluid maintenance.
Standard 2. IV fluid prescription
There was 100% adherence to the IV fluid prescription containing details of the type of fluid, volume and rate to be administered.
Standard 3. IV fluid management plan
Most IV fluid maintenance was initiated on inpatient wards, in 148 cases, with the remaining 85 being split as 59 in ED and 26 in admissions areas.
For patients receiving more than 24 hours IV fluid maintenance, 54% (40/74) had an IV fluid management plan. Standard 3 only applied if receiving IV maintenance fluids for more than 24 hours, so was not relevant for 159 patients.
Standard 4. Details of IV fluid management plan
The IV fluid management plan included details of the fluid and electrolyte assessment in 38% of patients, of fluid and electrolyte prescription over the next 24 hours in 48% of patients, and the monitoring plan in 15% of cases.
There was no fluid balance monitoring in place for most patients (124/233) and the fluid balance record was incomplete in a further 40 patients.
Standard 5. IV fluid resuscitation
IV fluid resuscitation was administered to 102 patients at any time (68 in ED and 34 on a ward). There was a documented cause of fluid deficit in 57% (58/102) of patients.
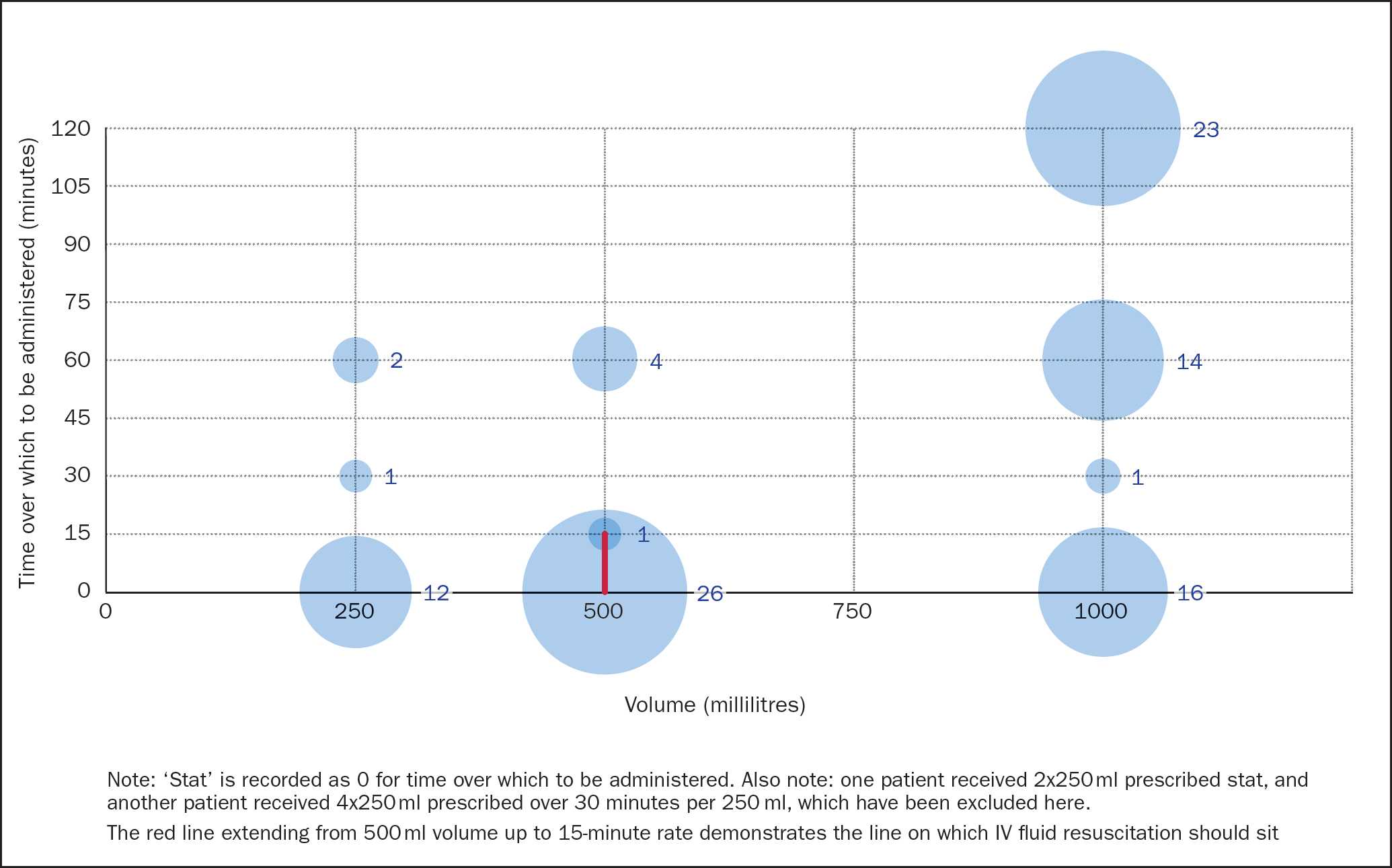
A 500ml crystalloid fluid bolus was administered in 25% of patients. The most common fluid composition prescribed for IV fluid resuscitation was 0.9% sodium chloride, in about 70% of patients, with Hartmann's solution/compound sodium lactate making up the remaining 30%. The most prescribed fluid bolus volume was 1litre, the most prescribed rate was ‘stat’ (immediately), and the most prescribed fluid bolus volume and rate combination was 500ml given ‘stat’ (Figure 3).
Standard 6. ABCDE reassessment
There was no documented reassessment in 48/102 patients, a documented reassessment within 6 hours in 18/102 patients, and an immediate reassessment in 36/102 patients. Of the patients who were reassessed, 9 were reassessed using an ABCDE approach, and 45 had evidence of a non-ABCDE reassessment.
Standard 7. Expert help following >2000 ml IV fluid resuscitation
Additional fluid resuscitation was administered in 25/102 patients, and 8 of these required >2000 ml IV fluid resuscitation. In 7/8 (88%), senior (ST3+) help was sought within 1 hour.
Standard 8. ABCDE reassessment after additional fluid boluses
Three of 25 patients requiring additional IV fluid resuscitation had ABCDE reassessment.
Standard 9. Expert help following >2000 ml IV fluid resuscitation
One patient displayed signs of shock despite adequate IV fluid resuscitation, and senior (ST3+) advice was sought for this patient within a 30–60 minutes window.
Standard 10. Initial IV fluid maintenance prescription
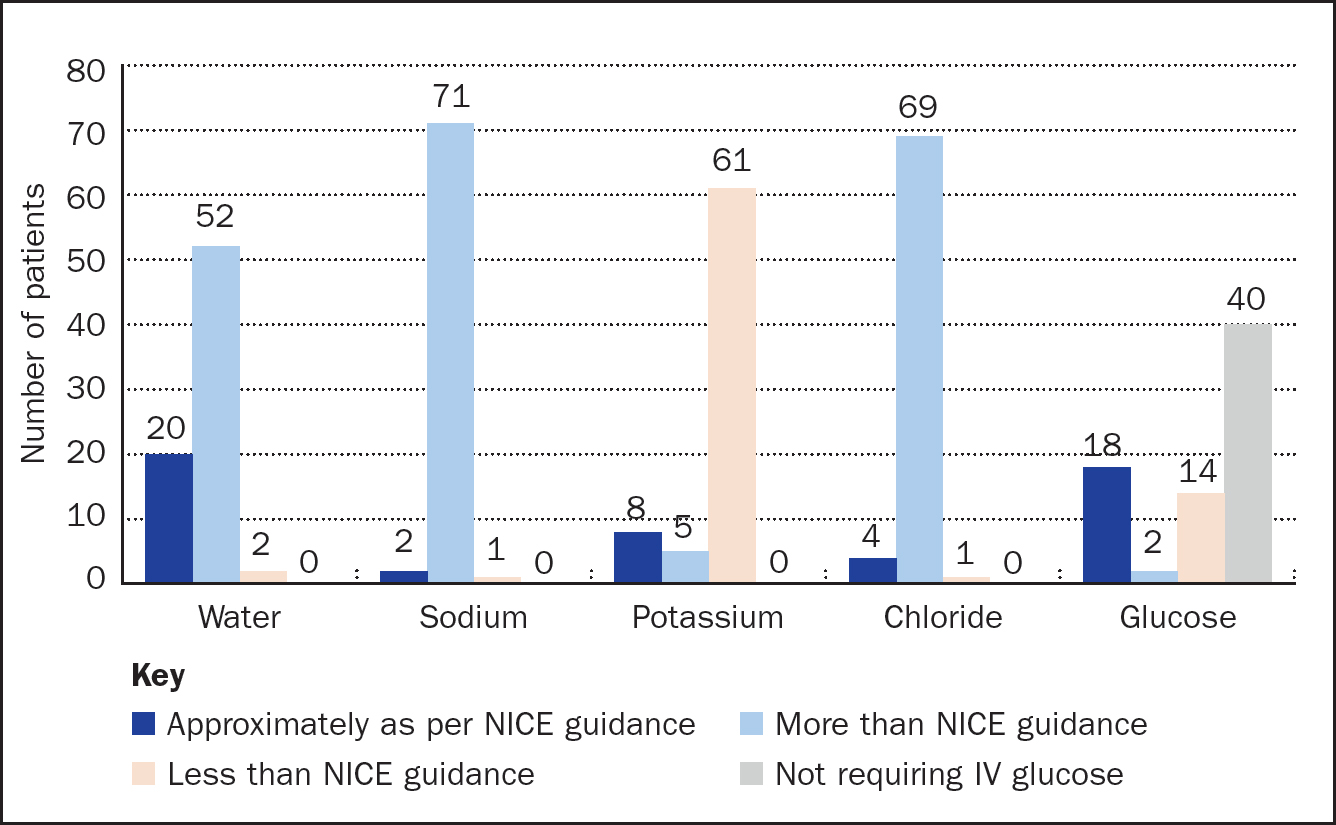
Regarding fluid maintenance, 74/233 patients were administered more than 24 hours IV fluid maintenance. Initial IV fluid maintenance prescription was restricted to 25–30ml/kg/day of water in 27%, approximately 1mmol/kg/day of potassium, sodium, and chloride in 11%, 3%, and 5% respectively, and approximately 50–100g/day of glucose, to limit starvation ketosis, in 53% (Figure 4).
The most prescribed initial maintenance IV fluid was 0.9% sodium chloride, in 127/233, followed by Hartmann's solution in 83/233, with the remaining 23 fluids including 5% dextrose, and fluid combinations with added potassium.
Standard 11. IV fluid prescription adjustment in obese patients
There was a weight documented on the prescription chart in 137/233 patients, which was within 1 week prior to the IV fluid maintenance prescription in 110/137 patients, not current in 25/137 patients, and not recorded on the drug chart at the time of initial IV fluid maintenance prescription in 2/137 patients. There was no weight documented on the drug chart at all in 96/233 cases.
In obese patients receiving IV fluid maintenance for more than 24 hours, no prescription adjustments were made in 7/13, and it could not be assessed whether adjustments had been made in 6/13. IV fluid prescription was adjusted to ideal body weight in 67% of obese patients, but expert help was not sought for the 3 patients with a BMI over 40.
Standard 12. Replacement/redistribution considerations
A total of 55 patients were deemed to have complex challenges related to fluid replacement/redistribution; 34 of these had senior (ST3+) input within 4 hours, 9 had senior input within 4 to 8 hours, and 11 had no evidence of timely senior input (relevant data for one patient were missing).
The reason for IV fluids was considered in most patients, however 51/255 had no clearly documented reason. Commonly documented reasons included dehydration in 58/255 and sepsis in 32/255.
Discussion
Target adherence of 95% was only achieved for standards 2 and 9, with most remaining standards showing an adherence level below 50% (Table 3).
| Standard | Adhererence (%) | |
|---|---|---|
| 1 | Fluid and electrolyte needs assessed prior to IV fluid prescription | |
| ■ Resuscitation | 21 | |
| ■ Maintenance | 26 | |
| 2 | IV fluid prescription | |
| ■ Type of fluid | 100 | |
| ■ Rate of administration | 100 | |
| ■ Volume of fluid | 100 | |
| 3 | IV fluid management plan (>24 hours) | 54 |
| 4 | IV fluid management plan | |
| ■ Details of fluid and electrolyte prescription | 48 | |
| ■ Details of assessment | 38 | |
| ■ Details of monitoring plan | 15 | |
| 5 | Patients in need of IV fluid resuscitation | |
| ■ Cause of fluid deficit identified | 57 | |
| ■ Fluid bolus of 500ml crystalloids given over <15 minutes | 25 | |
| 6 | Patients receiving fluid resuscitation reassessed using ABCDE approach | 9 |
| 7 | Patients receiving >2000 ml crystalloids and still need fluid resuscitation receive expert help | 88 |
| 8 | Patients not had >2000 ml crystalloids and require further bolus after reassessment are reassessed after further bolus | 12 |
| 9 | Patients showing signs of shock receive expert help | 100 |
| 10 | Initial IV fluid maintenance including: | |
| ■ 25–30 ml/kg/day water | 27 | |
| ■ lmmol/kg/day sodium | 3 | |
| ■ lmmol/kg/day potassium | 11 | |
| ■ lmmol/kg/day chloride | 5 | |
| ■ 50–100 g/day glucose | 53 | |
| 11 | Adjusted IV fluid prescription to ideal body weight | 67 |
| ■ Expert help sought if BMI>40 | 0 | |
| 12 | Expert help sought <4hours for patients with complex fluid/electrolyte redistribution issues/imbalance | 63 |
Beginning with standard 1, poor adherence to assessment of fluid and electrolyte needs was identified, suggesting initial patient assessment regarding IV fluids is not being completed as comprehensively as it should be from the NICE guidance.
The importance of fluid and electrolyte assessment, prior to IV fluids prescription, cannot be understated. First, it may indicate a patient does not require IV fluids, but is instead suitable for oral replacement. In patients who are assessed and found to require IV fluids, it is also key for identification of whether a patient requires IV fluid resuscitation or maintenance. Furthermore, having a baseline measure of fluid and electrolyte requirements allows targets to be set, and progress towards these monitored over time. No documented baseline may make it difficult to assess patient progress, and the efficacy of an IV fluid management plan, making it more challenging for clinicians continuing the care of a patient to develop an ongoing IV fluid management plan.
Poor initial assessment of fluid and electrolyte requirements links to the poorly completed ABCDE reassessment (standard 6) in patients requiring IV fluid resuscitation. Potential reasons for poor ABCDE reassessment may be the reality of clinical practice and pressures faced by staff, meaning a comprehensive ABCDE assessment is not always made. However, this could also be due to a lack of education regarding assessing fluid needs, including the dangers of IV fluid mismanagement, which may not be fully appreciated, especially when IV fluid prescribing is so commonplace (Callum et al, 1999).
Assessment of fluid and electrolyte requirements also links to development of an IV fluid management plan, as without assessment of these, it is impossible to properly plan how requirements should be met over the next 24 hours. IV fluid management plans should include details of fluid and electrolyte prescription over the next 24 hours, details of assessment (U&Es (urea and electrolyte levels), blood tests, weight, fluid balance), and details of the monitoring plan, to support ongoing patient care.
Poor IV fluid management plans may contribute to patients receiving more sodium than required, but not enough potassium; a finding shared by previous audits in other NHS trusts (Jordan et al, 2015). This raises the question of why prescribers prescribe the fluids they do, most commonly 0.9% sodium chloride or Hartmann's solution. This may be related to lack of knowledge regarding fluid compositions, including the range available, and may be an area where targeted educational intervention would be helpful. There may also be issues with availability of certain fluid compositions, making it more challenging for prescribers to correctly meet a patient's fluid and electrolyte requirements if alternative and better-balanced fluid compositions are not available. It is also important to consider that although IV fluid electrolyte requirements may not have been met, oral intake of fluids was not assessed, and this may also have an impact on the actual water and electrolyte input for each patient.
There may also be an interplay between fluid balance monitoring and IV fluid management plans, as poor plans may negate the importance of fluid balance monitoring and conversely no fluid balance monitoring may contribute to poor plan development. Fluid balance monitoring should be completed for every patient receiving IV fluids, but there may be a vicious cycle at play with poor communication about the requirement for fluid balance monitoring, or poorly documented fluid balance, leading to it being reviewed less often and therefore completed less often, and equally if it is not reviewed often then it may be completed less often as it is not perceived to be important. This highlights the importance of shared management plan discussions between physicians and nurses, to ensure a high level of patient care.
IV fluid resuscitation was often prescribed as ‘stat’ rather than ‘<15 minutes’ (within 15 minutes) and this may be regarded as poor prescribing practice, as ‘stat’ does not define a set time frame. At the trust in question, even if ‘stat’ is considered to mean as quickly as possible, a limitation of the fluid pumps is that they can only deliver a maximum rate of 1200 ml/hour, so cannot administer 500ml within 15 minutes. Therefore, to meet this standard, free-drain fluid bags would be required. If a strict timeframe of less than 15 mnutes had been required, then this would have meant 0% adherence to standard 4b.
The importance of prescribers and nurses in IV fluid administration and management
Although IV fluid prescription and administration may appear to be two separate processes, they are intricately interlinked and require effective communication and teamwork between prescribers and nurses. Prescribers take primary responsibility for the selection of IV fluids, but nursing teams have a crucial role in the assessment of a patient's fluid status, response to fluid therapy, and discussion with clinicians regarding ongoing IV fluid management (Guest, 2020). As a result, it is important for discussions to exist between prescribers and nurses regarding IV fluid management, as not only does this support evidence-based decision making, but also supports development and fulfilment of IV fluid management plans.
Comparison with available literature
This audit is the largest published to date regarding the NICE guideline CG174, including 255 patients and 335 separate IV fluid prescriptions. Reviewing data from previous studies, in combination with this project, there is room for improvement regarding adherence to the NICE guideline overall.
As discussed, this project found generally poor adherence to the NICE guideline, with only audit standards 2 and 9 meeting the target adherence of 95%. This is consistent with findings from previous studies, and may be due to poor awareness of the NICE guidance, prescribers and those administering not having adequate knowledge regarding IV fluids, and trivialisation of IV fluid prescribing and fluid balance, as suggested by previous work (Sansom and Duggleby, 2014; Mishra, 2018).
A previous audit completed at Royal Liverpool and Broadgreen University Hospital NHS Trust (Mishra, 2018), was similar in that IV fluid management plans were generally poorly completed. However, in contrast, the trust examined here was poorer with adherence to standard 1, where the Liverpool trust recorded 72% adherence.
Limitations
Accurate documentation in patient notes was relied on for data collection. If documentation was poor or incomplete, then it may have appeared that procedures, such as ABCDE reassessments, were not completed and could result in lower adherence to standards being noted in the audit than was actually the case. Furthermore, if documentation was not accurate, or timings of notes and prescriptions did not match up well, collaborators were required to apply a degree of their own interpretation of the information available. Other limitations relate to areas in which data collected were not extensive. For example, only the initial IV fluid bag was recorded for IV fluid maintenance standards.
Recommendations
Educational interventions
Several articles in the literature have documented the need for educational interventions regarding IV fluid prescribing, yet there are few follow-up articles detailing where these have been implemented (Powell et al, 2013; Howell and Patel, 2014). Examples of interventions that have shown benefit include the use of summary cards attached to lanyards worn by prescribers and a combination of formal and informal ward-based teaching sessions (McMenamin et al, 2016; Mishra, 2018).
In Northern Ireland, specialised fluid prescribing charts are used (Dowd and Robinson, 2015). These charts begin with fluid balance monitoring, often completed by nursing teams, followed by a step-by-step IV fluid prescription chart, including a table detailing the composition of commonly prescribed IV fluids, a fluid prescription advice section based on the NICE guideline, and a column for the prescriber to record IV fluid indications.
This is similar to adult IV fluid charts implemented in Hampshire Hospitals NHS Foundation Trust in 2014, which were popular with all staff groups (Jordan et al, 2015). Following their implementation, that trust found improved documentation of indications for IV fluids, improved daily electrolyte monitoring, and more ‘correct’ IV fluid volumes. However, there was a deterioration in meeting sodium requirements, with more patients receiving too much sodium, and there was no change in meeting potassium requirements, with patients generally receiving too little.
A similar intervention that may improve IV fluid documentation is the use of daily review template sheets, with sections to prompt fluid and electrolyte assessment, and a complete IV fluid management plan (Bewlay, 2016).
It is clear from the literature that educational interventions must be targeted at multiple levels, and to both prescribers and those administering IV fluids, for enhanced overall outcomes (Powell et al, 2013; Mathur et al, 2020). Therefore, ahead of the next audit cycle, two interventions are planned, targeted at both prescribers and administrators of IV fluids, in addition to supporting system development.
The first intervention will be an IV fluid prescribing workshop, provided to final year medical students during transition to clinical practice at the trust. This workshop will aim to improve confidence and competence in assessing patients for IV fluid needs, and support evidence-based decision making for IV fluid prescriptions. In a different trust, this style of intervention was not found to provide much benefit initially, but after further sessions and in combination with other interventions, contributed to improved adherence to audit standards (Cunningham et al, 2016).
The second will be a workshop provided to those most likely to be involved in the administration of IV fluids, such as nursing teams, at the trust. This workshop will more specifically target standards assessing fluid balance, discussing the importance of nursing teams in IV fluid management, the importance of fluid balance monitoring, and the importance of working with physicians to develop shared management plans.
Finally, there will be ongoing discussions with information technology teams to support design of electronic prescribing software, particularly regarding prescribing IV fluids.
Conclusion
Baseline adherence to NICE CG174 at the trust examined here requires improvement. Interventions should target standards where adherence was found to be particularly poor, including patient assessment and reassessment, and meeting electrolyte requirements. Interventions planned before the next audit cycle include workshops for prescribers of IV fluids and those administering them, and accelerating systems change for electronic prescribing of IV fluids.