
The 2015 Shape of Caring report (Willis, 2015) advocated a teaching model that championed coaching and peer learning entitled ‘Collaborative Learning in Practice’ (CLiP) (University of East Anglia (UEA), 2014). The Standards to Support Learning and Assessment in Practice (SLAIP) (Nursing and Midwifery Council (NMC), 2008) stated that students are required to be mentored by a registered nurse who has undertaken an NMC-approved programme and the nominated mentor must have been available for 40% of the students' placement time in order to complete a valid assessment.
Large numbers of students in placement areas can prove onerous for mentors (Huggins, 2016) and can adversely affect student satisfaction (Vinales, 2015). Owing to the increased numbers of new learners requiring placements, there is pressure on the placement circuits and the demands placed on mentors to support students and learners has increased. Mentors are often required to support up to three students per placement and ensuring quality learning experiences, coupled with the need to deliver safe patient care, has often proved difficult. Therefore, in a climate of an evolving nursing workforce and the introduction of roles such as the nursing associate, it is essential to examine the current mentorship model.
The NMC Standards for Student Supervision and Assessment (SSSA) (NMC, 2018) have mandated the abolition of mentors in favour of three new roles: academic assessor, practice assessor and practice supervisor. An NMC-approved course will no longer be required in order for registered professionals to supervise students. Furthermore, reform of the way in which students are taught in clinical practice is implicitly recommended in the form of a coaching approach. It is anticipated that both practice supervisors and practice assessors adopt a coaching approach to teaching and minimise the use of direction and instruction.
Background
Experiential learning in clinical placement currently constitutes 50% of pre-registration programmes. Student satisfaction is often linked with having a sense of belonging and being a valued member of the team, as well as the availability of quality learning opportunities (Jokelainen et al, 2011). The Shape of Caring review (Willis, 2015) emphasised the fact that pressure on mentors may lead to inadequate support of students and acknowledged that the principles of the SLAIP standards (NMC, 2008) would be difficult to sustain.
The CLiP coaching model (UEA, 2014) was championed in the Shape of Caring review (Willis, 2015). The CLiP model proposes that a registered professional with experience of the clinical area assumes the role of coach. Typically, the coach will supervise a group of students of mixed experience who would be the directors of care for a designated group of patients. In addition, the coach provides feedback to the students' allocated mentor in order for them to formulate an assessment of their students' performances. Coaches encourage students to be the main providers of care and to problem solve and practise without full direction but under supervision. The benefit of the coaching model is that students will be able to think critically and be equipped to practise autonomously at the point of qualification.
In order to comply with the NMC's (2018) SSSA and to ensure that the student experience is maximised in the face of anticipated challenges, a derivative of the CLiP model that was originally developed by the University of East Anglia was used for the coaching pilot (UEA, 2014).
Design
In order to implement change that is sustainable, it is necessary to consider the use of a change-management model to provide structure to a change project (NHS Improvement, 2018). Plan Do Study Act (PDSA) cycles are widely used in healthcare (Coury et al, 2017) and are suited to projects that require multiple iterations. Consequently, the design of the coaching pilot was based on a PDSA approach.
Plan
A steering group consisting of university staff, senior nurses within the participating organisation and clinical placement facilitators (CPFs) was developed following the publication of the NMC's (2018) SSSA and in light of an upsurge of interest in coaching following the CLiP project (UEA, 2014). The steering group was responsible for agreeing the structure of the coaching pilot (Box 1) and concluded that, in order for the pilot to succeed, all participating staff would receive coaching training based on the GROW coaching model (Whitmore, 2009) (Box 2). It was also determined that a literal implementation of the CLiP model (UEA, 2014) was not feasible due to limited resources, so a bespoke coaching model that incorporated the key principles of CLiP was designed. The original CLiP model uses a day coach who is absolved of other responsibilities and whose sole remit is to oversee the student experience. Due to staffing and ward pressures, it was not feasible to use a day coach. Staff who were involved in the learning zone often had additional responsibilities beyond that of supervising students and the learning zone and were occasionally expected to attend meetings, which were not always held on the ward. However, another member of staff would then be expected to supervise the students temporarily to ensure safety. In addition, the original CLiP model also proposes the input of a clinical educator. However, the area used for the pilot did not have a clinical educator. Using a dedicated day coach and having input from a clinical educator would have likely benefitted the pilot but this was not possible.
| A section of the ward would acquire ‘learning zone’ status |
| Three students (one third year and two first years) would work together to lead patient care |
| A registered nurse would supervise the students and take on the role of ‘coach’ |
| Each student would complete a daily learning log to evidence their learning and achievement of skills |
| G: Goal. What would you like to achieve? |
| R: Reality. What is the situation? |
| O: Options. What do you need to help you achieve your goals? |
| W: Will. What will you do to achieve your goal? |
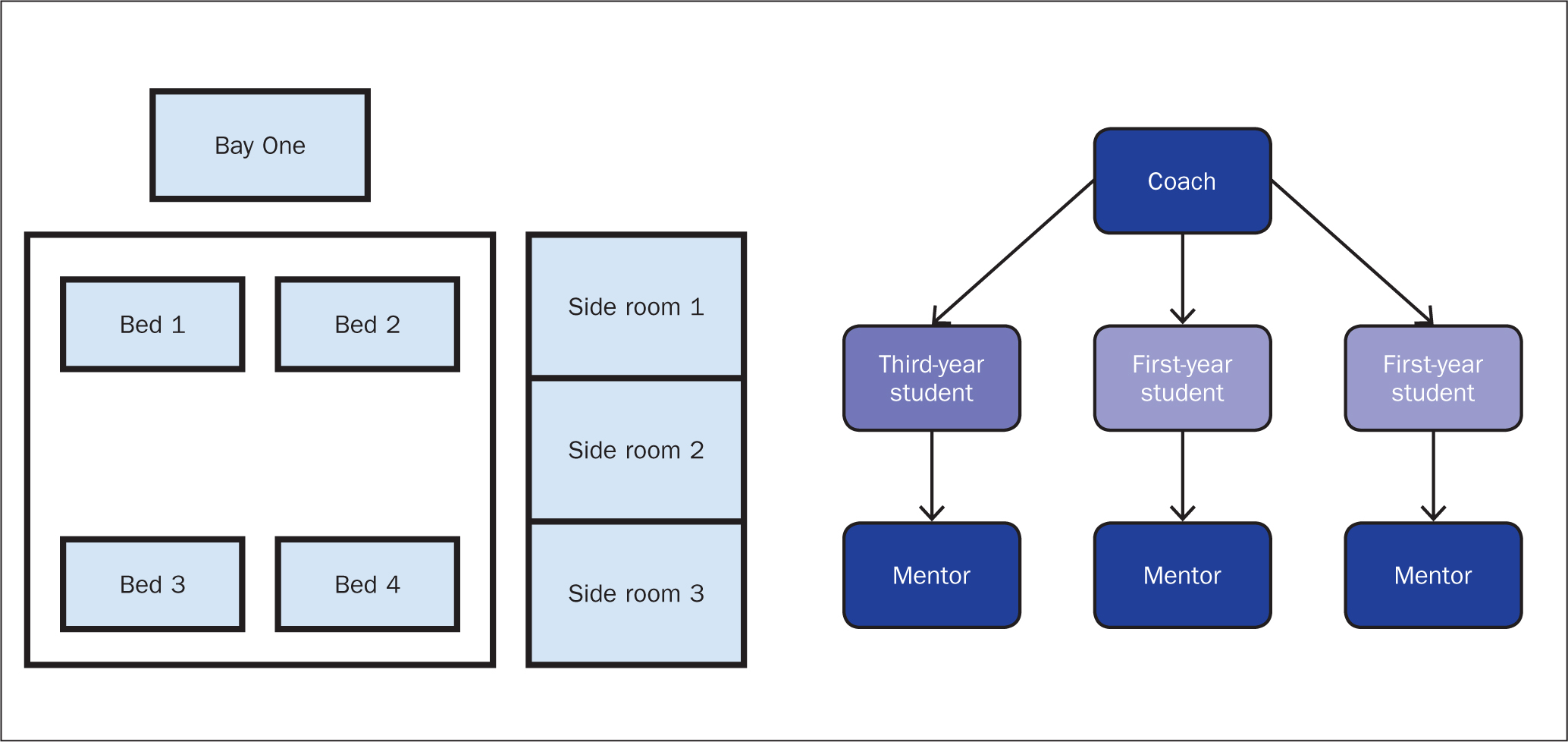
Evidence suggests that dedicated learning areas are successful in enhancing students' learning (Devereaux Melillo et al, 2014). Therefore, a section of the participating ward, consisting of seven low-acuity patients, was labelled the ‘learning zone’ (Figure 1). In order to mitigate risk, it was not deemed appropriate for the students to be the directors of care for acutely unwell patients or those with more demanding needs. Three students, consisting of one senior student and two junior students who were on placement at the same time, assumed control of the learning zone under the supervision of the coach, who had received GROW model coaching training (Whitmore, 2009). Full supervision of the students was required at all times to ensure patient safety and to minimise risk. The students involved had not had experience of working with the coaching model in previous placements—a fact that was taken into consideration when assessing them.
In terms of evaluating the pilot, the use of focus groups was deemed appropriate. As the coaching pilot was not intended to be a research project, the focus groups were for evaluative purposes only.
The aim of the pilot was to initially address questions that had been raised following examination of reports including the Shape of Caring (Willis, 2015), such as:
Do
In order for any change project to be successful and sustained it is essential that all individuals involved understand the aims and objectives (Alvesson and Sveningsson, 2015). In order to achieve this, ward staff participating in the pilot as a coach not only received comprehensive coaching training but were also aware of the need to innovate and reform practice. The project was championed by the ward matron and staff, regardless of role and seniority, were informed of the learning zone and the needed to be considerate to the fact that students would be directing care.
During the pilot, frequent visits were made by academic staff from the participating university and also the CPF for the clinical area. Logistical issues such as coordinating off duty and ensuring that students still worked a sufficient amount of time with their mentors while participating in the pilot proved problematic on occasion. Students were also required to work set shifts in order to ensure that three students were on duty at the same time. During the pilot, nursing assistants did not work in the learning zone. With the coach, one senior student and two first year students it was considered safe not to use a nursing assistant, although when the area experienced periods of pressure there was flexibility in this, and they could be called upon when necessary. As the first-year students were in their first clinical placement, they were expected to perform fundamental care tasks, to aid their development and learning.
In addition, the students received appropriate preparation through a presentation that stated the rationale and organisation of the pilot. As the students were not expected to coach themselves to the extent of the registered staff, they did not receive the coaching training in the same level of detail.
Study
Two focus groups were held at the conclusion of the coaching pilot in order to evaluate its effectiveness. The focus groups were conducted by the CPF who was not based on the ward involved, which ensured some impartiality and discussions were recorded through note taking by the CPF. Focus groups are considered to be an effective way of gathering qualitative data (Stewart and Shamdasani, 2015). Although focus groups can provide a rich form of data, there is also a propensity for the discussion to be led by more assertive members of the group (Casey and Kreuger, 2015). Consequently, it was deemed necessary to have two focus groups: one consisting of ward staff and one comprising the students in order to generate honest discussion and dialogue.
Both of the focus groups were held on the ward that participated in the pilot. Ideally, focus groups should be held in a neutral location, which may lend itself to a more open discussion (Tong et al, 2007). However, due to limited resources this was not feasible in this case, and both focus groups were carried out in identical conditions on the ward.
Each focus groups took 45 minutes and aimed to ascertain whether the pilot compromised or enhanced the student experience and whether organisational or logistical issues hindered the pilot. Mentor satisfaction and the efficacy of the preparation that ward staff received was also explored.
Act
Findings from both the student and mentor focus group determined that the coaching pilot was successful overall. The introduction of a learning zone was positively received and staff who participated in the coaching role were able to effectively use the GROW coaching model (Whitmore, 2009).
The student experience was positive overall but there was poor compliance with completion of a learning log. The learning log was proposed in the original CLiP model as a means for the student to reflect on their experiences and to demonstrate to their mentors that they have achieved their learning outcomes. However, students felt that it was an additional workload that they did not deem necessary. There was also poor compliance from coaches in completing the learning log as they felt that the practice assessment document was sufficient in confirming that students achieved their learning outcomes. Future iterations of the pilot will emphasise the importance of the learning log as a method for students to demonstrate that they have achieved competency and can evidence their learning outcomes.
For future cycles there will also be a need to consider providing extra support to the ward staff who arrange student off duty. Students were concerned about the lack of time working directly with their mentors and balancing this with the need to arrange off duty in a way that fitted in with the coaching pilot, and this proved problematic on occasion.
Change can only be considered if it becomes embedded, sustained and results in a cultural shift (Gage, 2013). Therefore, a second cycle of the coaching model will resume in the same placement area, in addition to a further roll-out across two similar wards, with the intention that repeating the coaching model for a second time will provide familiarity and an increased chance of sustaining change.
Findings
During the student focus group, particular attention was paid to the responses of the third-year students as they had the necessary experience to provide comparison between the existing mentorship model and coaching:
‘It made it the best placement I have ever had. I was nervous starting, but I feel so much more confident and have loved working with my team.’
‘It's been good, and I've learned a lot. It made me feel more relaxed knowing I could turn to a third-year student if I needed support. I've been able to do a lot of skills in the learning zone.’
Students were unanimously positive about working in a dedicated learning zone and stated that being coached allowed them to develop their problem-solving and leadership skills.
The second focus group, consisting of registered nurses involved in the pilot, raised minor concerns of the issues that they encountered:
‘There were positives and negatives. The third-year students had no knowledge of the specialty so it was difficult for them to lead a team at first. The first-year students were also on their first placement and some had no care experience at all.’
Regarding the logistics and organisation of the coaching pilot, the ward lead concluded:
‘It increased my workload at times as the students didn't like working set shifts and wanted to swap their duty. We had to refuse their requests to swap or the project would not have worked.’
Despite this it was concluded that none of the aforementioned issues were insurmountable. Furthermore, it was also concluded that a period of acclimatisation before starting the coaching model would ease student anxieties and allow them to become accustomed to the routine of the ward.
However, all staff that participated in the coaching role concluded that the students' development was evident and that they were able to assess the students' competence more clearly:
‘The students had more responsibility. It was nice to see their confidence and leadership skills develop. I could clearly see how well they were performing, and it helped me to assess them better.’
Discussion
Having evaluated the coaching pilot, several themes have emerged. Coaching, as opposed to mentoring, is a preferred teaching method among senior students, while junior students preferred a blended approach of both mentoring and coaching. Senior students perceived that coaching gave them autonomy and they were able to develop leadership skills as a result. Although the junior students enjoyed participating in the pilot, they shared the opinion that a more personal and directive approach, combined with the coaching, would have been beneficial. The junior students had very limited care experience before commencing the pilot and believed that direct learning from their nominated mentor would have been of benefit, in addition to the coaching model. Smith (2017) stated that although coaching is beneficial and allows individuals to achieve their learning outcomes, a blended approach of both coaching and mentoring can enhance learning further.
The ward staff who participated in the pilot said they generally enjoyed the experience, which was different to their usual experience with mentoring and assessing students. Mentors stated that the pilot meant that it was easier to assess students' competence because the students were given more responsibility and mentors were able to clearly see how they overcame difficulties and solved problems without being instructed. Mentors did not believe that the lack of use of the learning logs hindered them as the practice assessment document was comprehensive enough and the students had it in their possession each shift so were able to approach their mentors with it on a daily basis in order to demonstrate their learning.
In terms of addressing the aims of the coaching pilot, it was concluded that it is feasible to apply the coaching model to placement areas. Although the CLiP model (UEA, 2014) was specifically advocated in the Shape of Caring review (Willis, 2015), not all NHS placement providers have the resources to apply the model in its most literal form, which is to have dedicated day coaches and clinical educators. However, CLiP derivatives that still use the core principles of peer learning and coaching can be applied to any placement area, providing that there are students of mixed levels of experience. Although the coaching pilot encountered minor difficulties in ensuring that students fulfilled the SLAIP (NMC, 2008) standard assessment criteria and also participated in a model designed to complement the NMC's (2018) SSSA, it is anticipated that these difficulties will be overcome.
Following evaluation of the coaching pilot, it was also deemed appropriate to allow students a period of induction, with the rationale that their experience would benefit from having time to adjust to the ward culture and routine before commencing the coaching model. A blended approach can improve student satisfaction and also allow mentors the opportunity to work directly with their students, thus helping them to assess students. However, following evaluation of the pilot, the registered nurses who acted as coach concluded that it was obvious how competent the students were as they were expected to direct and deliver care and lead a team, all skills expected of newly qualified nurses.
Failing to fail students remains an issue in practice (Hughes et al, 2016); however, using a coaching model makes assessing a student's competency more straightforward, which may reduce the number of students who qualify but are not sufficiently skilled.
By ensuring that students work in small teams of no more than three, placement areas can ensure that there is not a saturation of students on each shift. The removal of the SLAIP (NMC, 2008) stipulation, that mentors must be available to students for 40% of the time, will also allow for more flexibility. Furthermore, by creating a designated ‘learning zone’ in each ward area, any individual with learning needs can participate in the coaching method. It is anticipated that nursing associates and newly qualified nurses who may require additional support can also participate in the coaching model, which will improve confidence, leadership skills and teamwork. The appeal of the coaching pilot is that students' learning is enhanced by working in a dedicated learning zone where their learning and development is a priority. However, further exploration is required to ascertain whether a blended approach of mentoring and coaching is more effective and also whether the coaching model can eradicate ‘failure to fail’.
Conclusions and recommendations
Coaching and peer learning can undoubtedly enhance the student experience on placement (Narayanasamy and Penney, 2014). However, the current method for mentoring student nurses is embedded in ward culture and it will take time and repetition to achieve sustained change. Students must also develop an awareness of coaching and peer learning, which can be achieved by higher education institutions placing an emphasis on this throughout the duration of pre-registration training. Coaching, peer learning and teamwork should have equal emphasis to clinical skills during simulation sessions and any future curriculum development should acknowledge coaching and the benefits of it on clinical placement.