

Following a number of patient safety incidents in elective surgical admissions, the general surgery department at Poole Hospital sought to improve prescribing practices in elective admissions and take steps to prevent similar errors recurring in future. Medical errors are estimated to contribute towards 1708 deaths a year in England (Elliott, 2021). Preventable adverse drug events are responsible for 20% of injuries or death to patients each year (O'Malley, 2007). Peri-operative prescribing errors have been described previously within otolaryngology patients, with documentation of medication histories being highlighted as one of many reasons for this (Rosenwasser et al, 2010).
The authors found that these errors predominantly affected frail patients who were taking multiple medications or those on medications that need to be given in a timely manner: for example, Parkinson's medications that, if missed, could have negative outcomes for the patient. These discrepancies have been shown in multiple studies (Beers et al, 1990; Cornish et al, 2005).
The literature suggests that improvements have occurred in some trusts; one method is by employing a prescribing pharmacist to collate a medication history and prescribe when a patient is initially admitted pre-operatively. Two studies have shown that medication errors decreased in number once this measure was initiated (Kantelhardt et al, 2016; Nguyen et al, 2020). Employing additional staff members requires significant financial input and, in a healthcare system that is already affected by financial issues. The authors sought to find cost-effective changes, because interventions are typically taken up on a wide scale if they require only simple changes that have no financial burden and are easy to implement.
The project described in this article aimed to look at the procedures from initial presurgical assessment throughout the journey until discharge, to determine whether any cost-effective, sustainable improvements could be implemented to prevent missed medication doses.
Methods
To investigate whether an elective general surgical patient had missed a dose of their regular medication, the authors looked at the patient's electronic prescribing record (Electronic Prescribing and Medicines Administration (ePMA)) to determine what medications had been prescribed and on what date and time this had occurred. ePMA is the Trust's local electronic prescribing system, which is a record of the prescription of medication doses, timings, frequencies and administration. The authors cross-referenced this information with the medicines reconciliation, a report of an individual's current medication regimen using community records and patient discussion, completed by the pharmacist on the patient's admission. The majority of regular medications are usually given by 10pm, so the general surgery department had a cut-off time of 10pm on the day of admission: if a dose was not administered by this time, it was recorded as a missed dose.
A baseline audit was performed for elective surgical patients over a 4-week period to gather a representative data sample of missed medication doses, as described, in those undergoing elective surgery in this time frame. The subsequent interventions thereafter were also assessed over a 4-week period. Changes were then made using the iterative Plan, Do, Study, Act (PDSA) cycle (NHS England and NHS Improvement, 2022). As laid out in the guidance, (1) a change is formulated, (2) carried out, (3) data collected on measurable outcomes and (4) then further changes may be planned (NHS England and NHS Improvement, 2022). Using this structure allows informative data to be collected on the effectiveness of an individual change.
During the project, COVID-19 affected the continuity of the data gathering, as elective operations had to be postponed, so, between the implementation of interventions 2 and 3, the collection of data was halted. Further data were gathered once elective operations were running to initial capacity.
To create a driver diagram, the authors simulated a patient's journey from pre-admission clinic, through admission, surgery and admission to the ward. During this time, we investigated each stage at which medications may be documented, prescribed and given by the healthcare team. By scrutinising the patient pathway, the authors identified both primary and secondary drivers behind the problem and from this, identified several potential interventions (Figure 1). Of these, following discussion with the pre-admission team, ward staff and theatre staff, the authors identified four interventions that would be reasonable and achievable to make:

- Intervention 1 introduced dose and frequency columns to the surgical pre-admission pro forma
- Intervention 2 allowed the pre-admission nursing team to prescribe a patient's medications prior to admission
- Intervention 3 ensured that all junior doctors had access to a functioning summary care record (SCR) card
- Finally, intervention 4 prompted junior staff to ensure that the correct medications are prescribed, once a patient has been admitted to the ward, via induction, teaching and visual reminders.
Intervention 1
The authors scrutinised the elective admissions booklet and how medications were being documented. They found that the table contained a single column for medication name, but had no columns prompting health professional to record dose, frequency or formulation. Therefore, this information, all of which is required to safely prescribe medications on admission, was often missing. This table was consequently modified, with columns added to record frequency, formulation and dose.
The goal was to have all medication information transcribed clearly and accurately documented on the pre-admissions pro forma for the admitting team, including the anaesthetist, surgeons and ward juniors, so that medications were prescribed correctly and in a timely manner.
Intervention 2
The second intervention focused on the presurgical admissions team, formed of nursing staff, and the process used in admitting a patient. The authors discussed their concerns and the initial audit with the pre-admissions team, who trialled nurse prescribers within the department; these were members of staff who worked in the pre-admissions clinic who were accredited prescribers, but had not previously been required to prescribe.
The proposed intervention was to have all medications prescribed at the pre-admissions appointment prior to admission, on the ePMA, and also to ensure that all suitable peri-operative drugs were suspended. It was the hope that not only would this improve efficiency, but also patient safety: it would meant that when the patient was admitted, the drugs would already have been prescribed in a controlled, unrushed environment, with plenty of opportunity to investigate doses/frequency with the GP in hours if required.
The pre-admissions clinic takes place 2 weeks before the date of surgery. There is therefore a small period of time over which medications may change; this led the authors to intervention 3, which would enable an up-to-date community medication record to be accessed.
Intervention 3
Junior doctors covering the ward in the evening are often bleeped by nursing staff to ensure medications are correct, especially if disputed by patients. Possessing a summary care record (SCR) card allows doctors to see GP records, including all current and discontinued medications, even out of hours when the GP practices are closed and therefore uncontactable. The third intervention aimed to ensure that all junior doctors had access to SCR cards: the hope was that this would result in a decrease in the frequency of missed medications due to an inability to contact the patient's GP or next-of-kin out of hours.
Intervention 4
To ensure that junior doctors covering the wards were aware of elective patients and the importance of ensuring that medications were prescribed in advance of admission, a teaching session was introduced at the beginning of every rotation. This took the form of a 5-minute talk during induction sessions, during which the process was explained, including how to gain access to SCRs, the use of pre-admission booklets and where to find them, and medications that it was important to withhold either pre- or postoperatively. This information was further endorsed with visual prompts in the junior doctors' office in the form of posters. These were welcomed by the surgical team and are sustainable within themselves.
Advanced care practitioners, who are present on the wards, may be a second option if junior doctors are not available; this is something that could be investigated with a further PDSA cycle.
Results
Each of the four interventions were introduced one after the other consecutively, and the authors re-audited after each change to assess its effectiveness.
The baseline audit (n=153) demonstrated that 9.8% of patients had missed a dose of medication. After intervention 1 (making changes to the pro forma), the percentage of missed medication doses after intervention 2 (n=128), enabling nurses to prescribe/suspend medication pre-admission, fell to 3.9% (n=5) (Figure 2), an improvement of 60%.
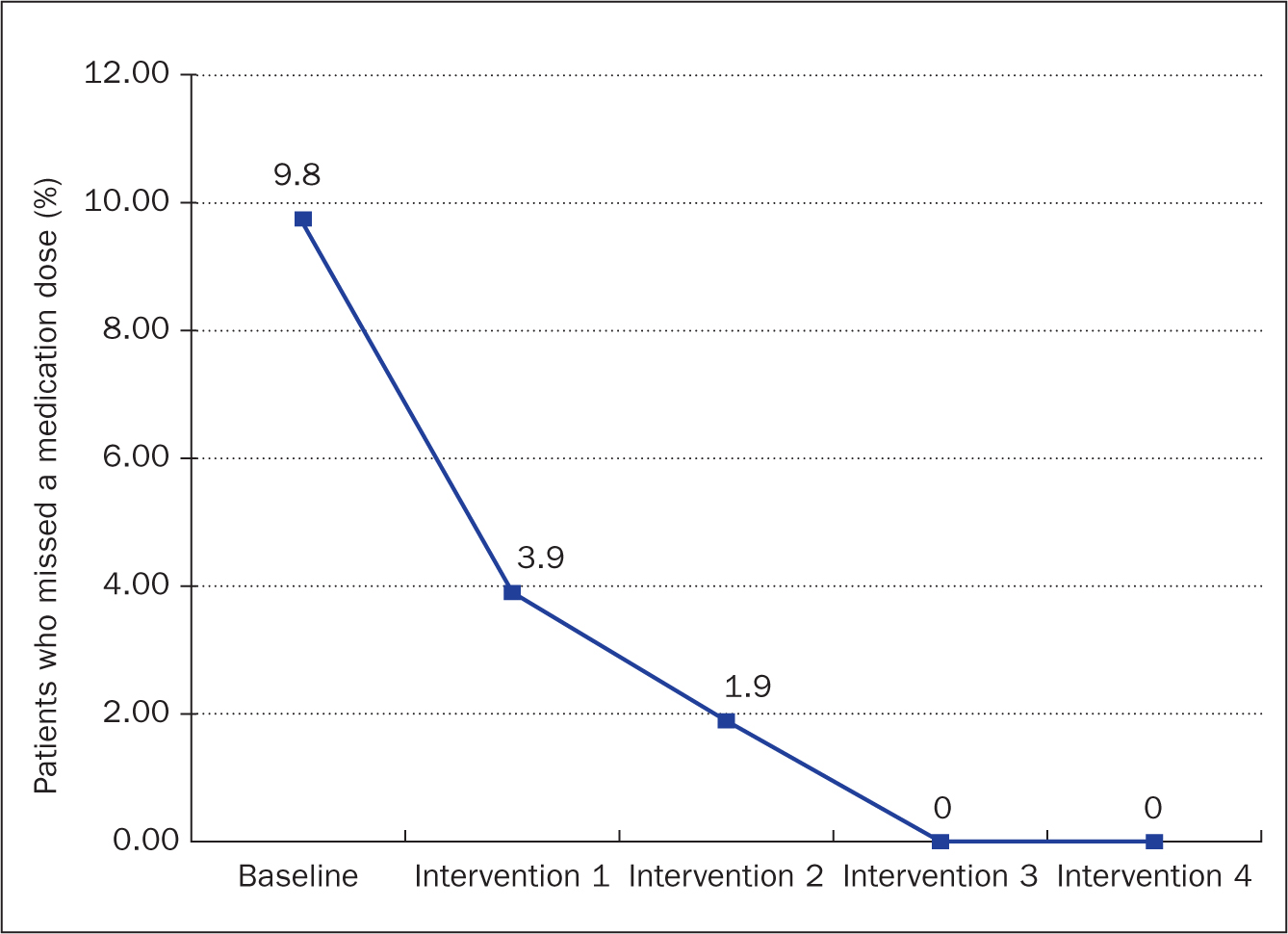
Pre-admission prescribing showed that two of the elective patients had missed doses of medication (n=106), just 1.89% (n=2) of the cohort. Results after ensuring SCR access (intervention 3) showed that of the patients admitted (n=137) 0% missed a medication dose. Following our final cycle (intervention 4), missed medication remained at 0%. Overall, we have seen a significant reduction from 15 patients a month missing a dose to none.
Discussion
This quality improvement project showed that simple interventions could have a significant impact on reducing the numbers of missed medication doses. The authors thoroughly interrogated the process that is currently in use using the driver diagram (Figure 1), changing parts of the process that were identified as potentially unsustainable, which were not financially dependent. Although it should be noted that the cost to the patient and organisation of drug errors should be considered when considering investment in quality improvement projects. This project used these simple alterations to established practices, which resulted in significant change, fitting in with the authors' need for sustainable interventions.
This project illustrated a range of different measures that could be used to help decrease prescribing errors in patients. However, on reflection, it has been deemed that two of the interventions are fully sustainable, these being the altered pro forma and the introduction of prescribing pre-admission by nursing staff. Two years later, both these interventions remain standard practice with elective surgical patients. These interventions are simple and required no financing by the Trust. However, they do increase the time spent with each patient by the pre-admission nursing staff. Although there was no need for additional financial resources to implement these interventions in the authors' Trust, this may not be the case for other trusts, where financial input may be required.
Intervention 3 now has less impact on new patients as a new care summary record system has been implemented since this project was completed. The new system allows all healthcare staff to gain access to a patient's previous medication records without the need for a specific card to log on.
Induction teaching for newly rotating juniors has been deemed not to be a sustainable change in the context of this project. Limitations have occurred from a lack of continuity, availability of staff for teaching and lack of time for teaching sessions. Therefore, the authors suggest that this system change is not maintainable, in its current state, after the project is complete. To ensure this intervention has lasting change, the authors suggest that this type of teaching could be included in a junior doctor's induction. They aim to complete a further cycle to evaluate the sustainability of the changes implemented.
To highlight the fact that the two interventions deemed to be the most sustainable and relevant to everyday practice are led by nursing staff shows the importance of nurse prescribing. If nurses are encouraged and supported to undergo training to gain prescribing qualifications, this project has shown that this brings benefits to patients by reducing drug-related errors. The pathway that elective patients follow provide an ideal opportunity – the preadmission stage – during which drugs can be prescribed in advance, a stage at which doctors are typically not involved. Advanced practice nursing roles have been developed within the NHS to increase the number of health professionals able to prescribe, which has helped to address workforce issues (Hill et al, 2021; Saunders, 2021). Nursing staff in these roles tend to stay under one clinical directorate for a longer period than junior doctors, who rotate every 4-6 months. Providing these nurses with the initial training regarding pre-operative prescribing would mean that fewer initial induction sessions would need to be provided, and therefore would ensure that intervention 4 is sustainable. Involving nurses in delivering such training sessions would further increase the sustainability of this intervention.
Further benefits to nurse prescribing have been described in many countries (Bhanbhro et al, 2011; Kilańska et al, 2021). Patients find it easier to access prescribing in primary health care, so having continuous access to medication in the community ensures that there are no missed doses of regular medications due to a lack of prescribers.
This project is therefore limited due to the fact that the authors' department relies on the pre-admissions team to have prescribing qualifications. This may, however, not be the case: nurse prescribers are not always routinely available in the authors' Trust on a daily basis, which is also likely to be the case in other trusts. In such circumstances, there would need to be some financial outlay to employ individuals able to prescribe as permanent staff members or to fund training of staff already working in the department, which may make this intervention less achievable. The need for such financial outlay can be a significant barrier to the implementation and ongoing provision of pre-admission prescribing of medication by nurses (Fox et al, 2015).
A comparison of costs between mental health nurse prescribers and independent prescribers (doctors or dentists) showed there were no significant differences in financial outlay (Norman et al, 2010), proving that this could be a cost-effective initiative that would help reduce hospital admissions and lead to shorter patient stays (Mitchell and Pearce, 2021). Indeed, a review of the patient pathway could look at the skill set held by nurses in the pre-admissions team, particularly the ability to prescribe, as well as identify how advanced roles can augment the patient journey and enhance quality performance indicators. These can then be used to underpin a business case for workforce transformation such as the initiatives described in this article.
The authors have shown that there are several points along the patient pathway at which medications may be prescribed, a task that can be undertaken by a variety of team members. The project has shown that supporting nurses to gain prescribing qualifications reduces the rate of medication errors. Organisations should look to support nurses who are keen to gain prescribing qualifications, which will promote better, safer practice.
During the course of this quality improvement project, COVID-19 presented a barrier to elective surgeries, the majority of which were cancelled. However, it was continued after elective surgeries were rescheduled, so that it spanned a period of nearly two years. Although no processes were changed during data collection, one limitation could be that those patients who had fewer comorbidities – and therefore fewer medications to prescribe – may have had their surgery postponed outside the time frame of this study. Further limitations could be the short time frame over which the patient data were gathered, the evening cut-off time of 10pm and this being a single-centre study.
Conclusion
This quality improvement project has shown that the use of an in-depth driver diagram can help identify simple, sustainable changes that can be made to a long-standing patient pathway that has benefits for patient outcomes.
The authors have shown that empowering nurses to prescribe at pre-admission stage can significantly reduce the percentage of patients who miss a medication dose. Ultimately, implementation of such an initiative must identify benefits for patients; it is also important to take into account whether such a change is cost-effective compared with the current practice of prescribing by junior doctors.
An initial financial outlay will be required to enable nurses to prescribe. However, this would be balanced by the decreased number of missed medication doses, which will in turn reduce the number of medical complications that can occur in elective surgical patients and reduce length of hospital stay, thereby reducing the cost of caring for these patients. The authors therefore propose that nurse prescribing should be encouraged, with education and support provided for nurses who are part of pre-admissions teams.
The authors aim to follow up this project by undertaking a further data collection exercise in 6 months' time when the changes have been in place for a significant amount of time. A further PDSA cycle will hopefully confirm the sustainability of the interventions over the longer term and that they have delivered lasting improvements.
KEY POINTS
- Prescribing errors are a common and easily preventable risk to patient safety in the inpatient setting
- Often, simple and cost-effective interventions can be put into place to help mitigate these risks if the prescribing pathway is interrogated carefully
- The emergence and increasing use of nurse prescribers is improving patient safety by decreasing medication errors and enhancing prescribing practices in the inpatient setting
CPD reflective questions
- Based on what you have read in this article, are there any ways in which you could make prescribing safer in your department?
- Do you think that nurse prescribers could improve patient safety in your department?
- If you already have nurse prescribers in your department, are they being used to their full potential? How can you empower them to improve prescribing practices in your department?