
Hospital-acquired pneumonia (HAP) is defined as a pneumonia that develops more than 48 hours after hospital admission. It affects approximately 1.5% of inpatients (National Institute for Health and Care Excellence (NICE), 2012). It is one of the most common healthcare-associated infections contributing to death and is estimated to increase hospital stay by up to 11 days (De Angelis et al, 2010). As well as increasing economic burden on hospitals (De Angelis et al, 2010), HAP carries significant morbidity and can increase mortality by 30-70% (NICE, 2012), especially among the elderly and frail. Immobilised patients and those with pre-existing lung conditions are at particular risk (Sopena et al, 2014). As guidelines for recognition and management of sepsis have been revolutionised in recent years, the early prevention of HAP becomes increasingly relevant. Preventing sepsis in the early stages by avoiding the development of primary infection has the potential to save numerous lives (Guiliano and Baker, 2020).
Background
It is widely acknowledged that quality improvement projects (QIPs) advance health care and are integral to reaching the targeted outcomes that provide best possible care for patients (Charles et al, 2019). As health professionals, it is important to actively reflect on ways to improve practice in order to deliver optimal services through continued learning and development (NHS England, 2019).
Significant work by Barbara Quinn, Dian Baker and colleagues in the USA found that non-ventilator associated HAP (NVHAP) was substantially under-reported due to problems with surveil-lance compared with that of ventilator-associated pneumonia (VAP) (Quinn et al, 2014). They looked at changes to basic nursing care, and their findings provided a strong foundation for hospital trusts elsewhere to consider how their nursing practices can be adjusted and improved to prevent HAP.
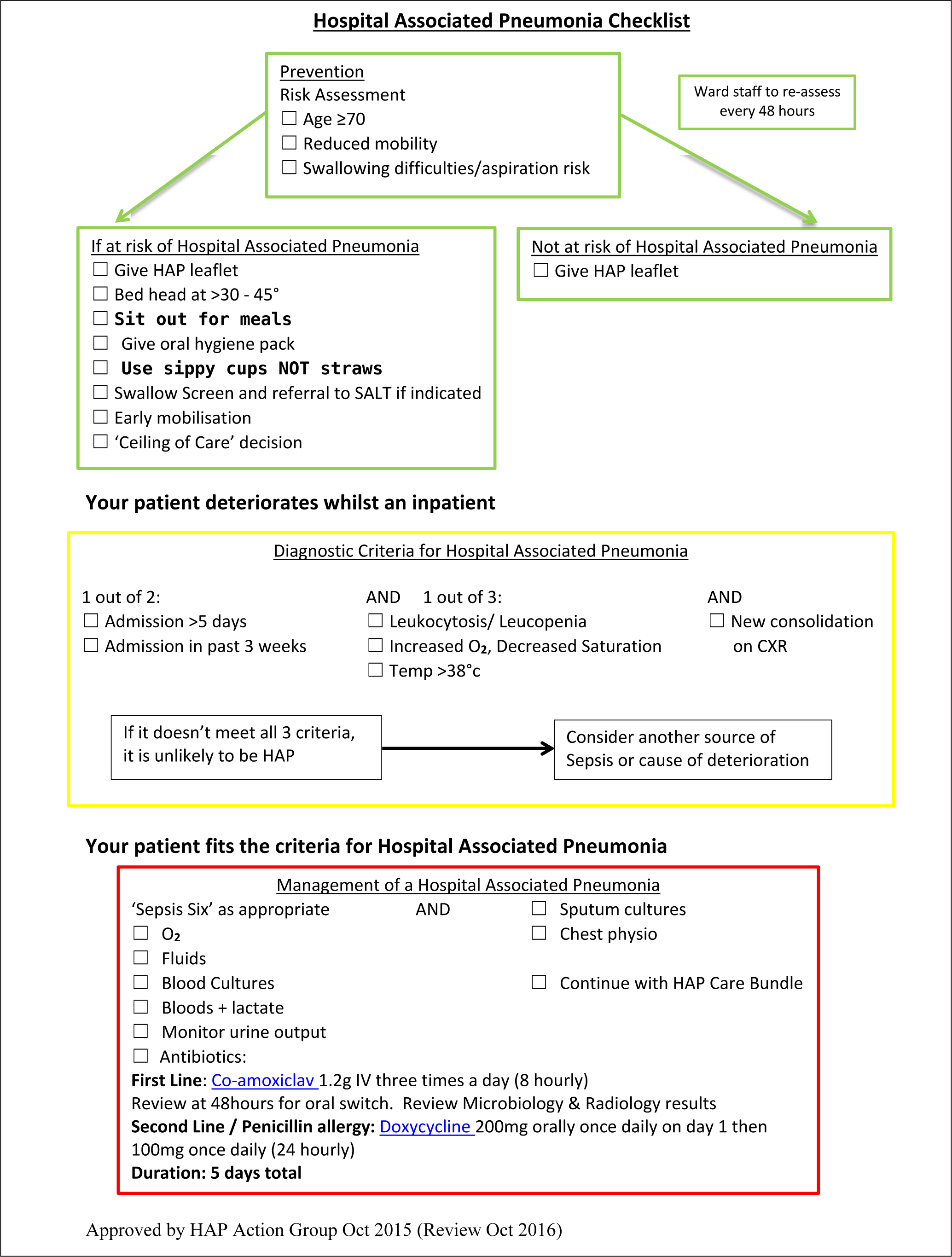
With this in mind, a checklist was produced at one hospital Trust in the south-east of England (Figure 1) with the aim of providing an accessible flowsheet for identifying patients at risk and recognising the symptoms of infection early, thereby helping health professionals to know when to initiate treatment. This QIP primarily focused on initial prevention, aiming to engage the nurses and allied healthcare workers who have most interaction with these at-risk patients and to equip them with simple and achievable measures that can be performed on wards.
Methods and predictions
The project was designed using guidance from the Healthcare Quality Improvement Partnership, in particular the guidance on development of audit tools and data collection in quality improvement (Dixon and Pearce, 2011). Three audit cycles were completed over a period of 6 months, allowing sufficient time between cycles for the introduction of interventions and allowing for a period of adjustment. The data were collected by medical students, based on a combination of their observations of patients on set days (both at mealtimes and on random occasions), together with information from patient notes. This provided snapshots, which were recorded on paper audit charts and collated for the three wards on those set days at the same time. The wards were not given advance notice on the audit days in order to reduce potential bias and gather a true representation of compliance with the preventive measures.
To evaluate the situation at the beginning of the project, a baseline audit was conducted in October 2016, which looked at 76 inpatients over 3 elderly care wards. It assessed five measurable domains, all shown to reduce risk of aspiration, and therefore risk of HAP. These included:
Guidelines were developed using the guidelines from the American Thoracic Society and the Infectious Diseases Society of America (2005) on the diagnostic criteria and prevention of HAP. More recent guidance from these bodies in 2016 commented on the 2005 publication, stating that little had changed in evidence for these strategies since 2005 (Kalil et al, 2016).
Most of the evidence behind the above measures is associated with reducing risk of aspiration. There are ample studies on prevention of HAP in ventilated patients (VAP), and in comparison the evidence for NVHAP is limited. More studies are required in this specific patient group (Quinn et al, 2014; Pássaro et al, 2016).
Numerous reports have shown a relation between poor oral hygiene and bacterial pneumonia (Talley et al, 2016). Therefore, during this project the speech and language therapist (SALT) team were involved in educating patients and staff about the importance of mouth care. The aim was to provide patients with oral hygiene packs containing toothbrush, toothpaste and mouthwash, and for those patients who could not perform their own mouth care, staff were encouraged to aid with teeth brushing.
Following the initial audit, the first four interventions were:
From these measures an increased awareness of the project among staff was predicted, leading to an improvement in efforts to comply with the measures.
The target group for this QIP were the ward nurses and healthcare assistants. This was due to this group having the most contact with the patients and therefore being best equipped to ensure the suggested changes were enacted. However, the QIP was not exclusive to this group and the education sessions also involved ward doctors, the SALT team, physiotherapists and ward support staff, with a view to ensuring widespread awareness.
The presentations given to doctors introduced them to the diagnosis and management arm of the checklist. Assessing improvements in these areas was beyond the scope of this QIP, but may be useful to target in future and would be aided by the checklist already provided in this project.
The checklist (Figure 1) had been developed prior to this project in 2015 by another team who had been unable to introduce it at the time. It had been approved by the hospital's HAP action group, and then reviewed by the same group in 2016 before this QIP in order to make sure that it remained in line with current best practice. The antibiotic guidance was taken from local Trust guidelines.
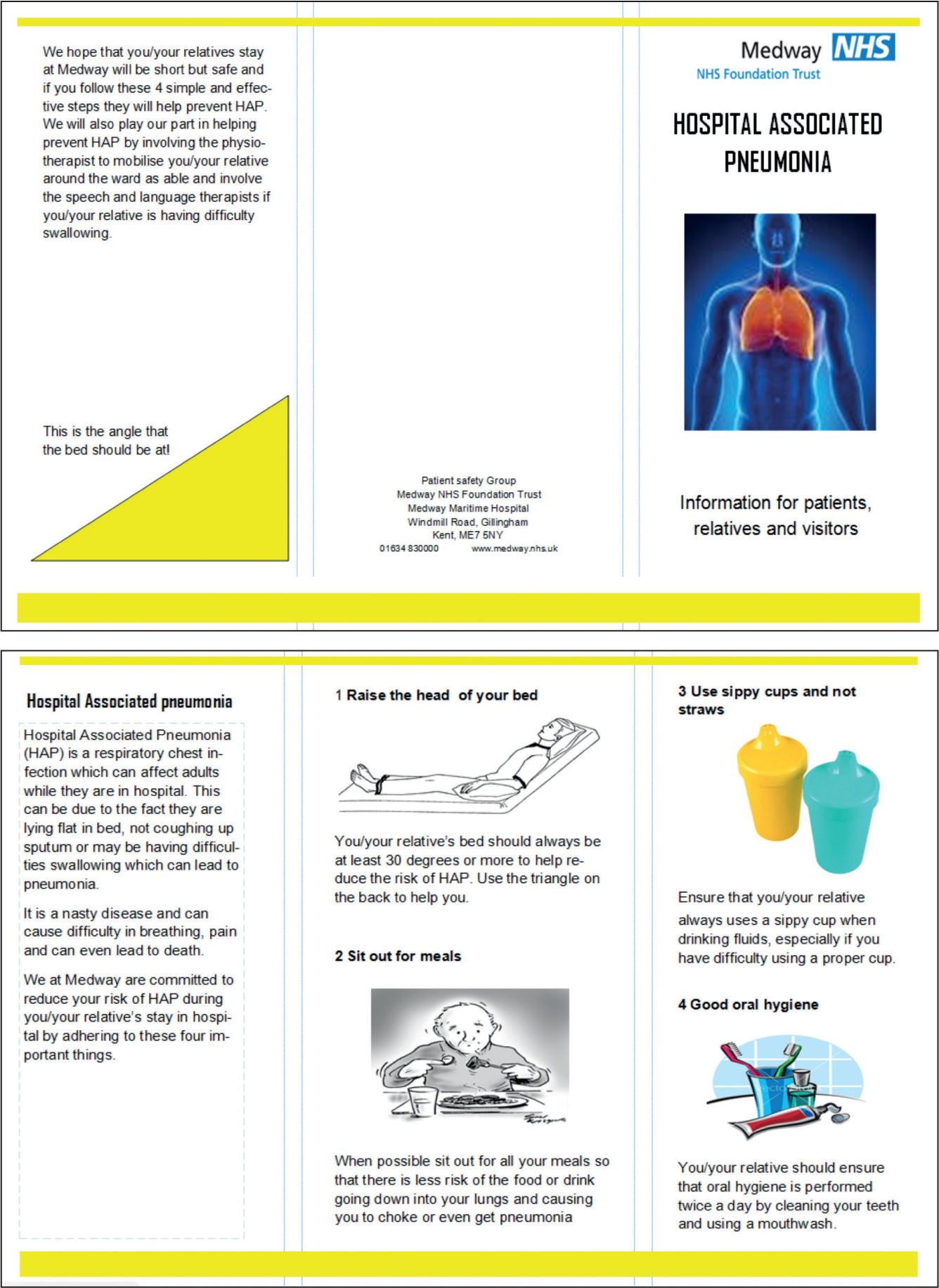
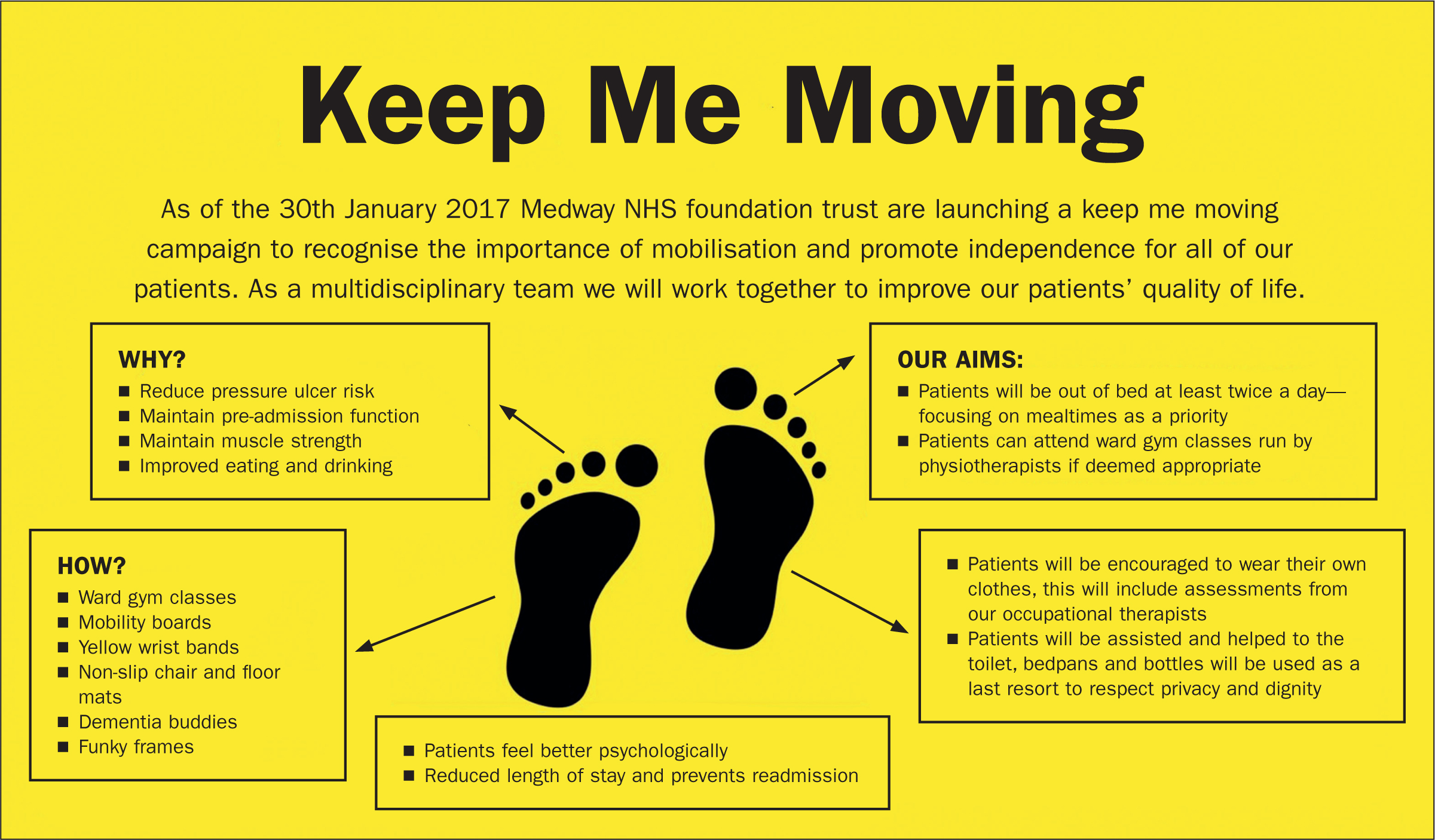
In January 2017, a second audit was completed to identify any areas that needed further work and any barriers to implementation. Following this a second round of interventions involved distributing leaflets (Figure 2) to all patients and their families (having discovered that this had not been done in the first cycle), and the distribution of oral hygiene packs. This coincided with a ‘Keep me moving’ poster campaign (Figure 3), which aimed to encourage early mobilisation and was being run by the physiotherapists and occupational therapists. Information on which patients were to be mobilised was gathered from patient notes. Because this is one of the domains that was initially assessed in the QIP, it is important to mention this intervention because it is also a known strategy for prevention of HAP. From here, it was expected that a return for the final audit in March 2017 would show an improvement in these additional areas.
Results
Table 1 shows the raw data collected in each audit. These are descriptive data and no statistical tests have been applied. Reasons for data recorded in the n/a (not applicable) column rather than yes/no columns include patients being flagged as nil by mouth, patients asleep, or having a flat bedhead but sitting in the chair, thus making the bedhead irrelevant. When calculating the percentages, these values were therefore excluded from the total.
| Cycle 1 (n=76) | Cycle 2 (n=77) | Cycle 3 (n=69) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes | No | n/a | Yes | No | n/a | Yes | No | n/a | |
| Bedhead >30 degrees | 49 (68%) | 23 (32%) | 4 | 39 (85%) | 7 (15%) | 31 | 40 (90%) | 4 (10%) | 25 |
| Out of bed for meals | 22 (31%) | 48 (69%) | 6 | 42 (60%) | 28 (40%) | 7 | 35 (52%) | 32 (48%) | 2 |
| Oral hygiene pack | No data | No data | No data | No data | No data | No data | 53 (95%) | 3 (5%) | 13 |
| Non-spill adult feeding cup | No data | No data | No data | 59 (77%) | 18 (23%) | 0 | 63 (91%) | 6 (9%) | 0 |
| HAP leaflet | No data | No data | No data | No data | No data | No data | 69 (100%) | 0 | 0 |
| Early mobilisation | 52 (72%) | 20 (28%) | 4 | No data | No data | No data | 50 (72%) | 19 (18%) | 0 |
| Use of straw (cycle 1 only) | 19 (35%) | 36 (65%) | 21 | ||||||
Data recorded as n/a (not applicable) if patients flagged as nil by mouth, asleep, or have flat bedhead but sitting in chair Patients recorded as n/a excluded from percentage calculations
Summary of results
Figure 4 summarises trends in the domains for which the most consistent data were obtained. In the first cycle, use of drinking straws (which are risk factors for HAP) was assessed rather than use of adult feeding cups (positive preventers of HAP), because these cups had not yet been distributed. Therefore the results were evaluated using the percentage of patients not using a straw (66%) as cycle 1 data, and percentage using a feeding cup in the next two cycles. As a result, there is an increase in appropriate drinking technique from 66% to 91%. A similar improvement is seen in the percentage of bedheads >30°, rising from 68% to 90% between cycle 1 and cycle 3.
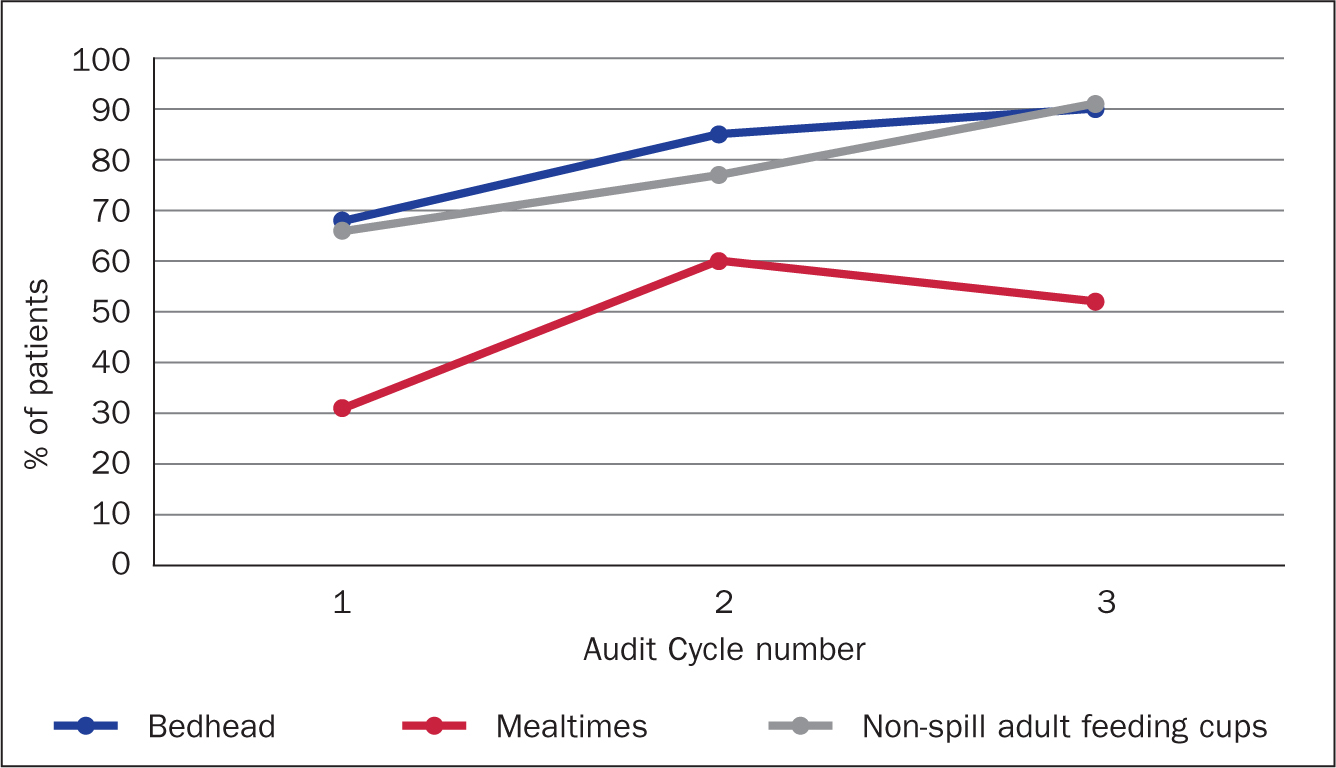
The number of patients sitting out of bed at mealtimes rose quite significantly between cycles 1 and 2, but fell between cycles 2 and 3. This was disappointing after the improvement of cycle 2, but could be explained by fewer staff on duty during the third audit, suggesting that fewer staff were available to assist patients getting out of bed. Despite this, there was an overall rise between cycles 1 to 3.
It was difficult to assess trends in oral hygiene because at the beginning it was found that mouth care was poorly documented in the notes, and the official oral hygiene packs were not distributed until late in the project, meaning there was no data for cycle 2. Another difficulty came in evaluating data about leaflet distribution because these were not officially handed out until the beginning of February 2017.
In addition to audits, a short staff survey was conducted in February comprising three questions:
Of 27 staff members working on the three wards on the day of cycle 2, there were 21 responses made up of 15 nurses, 3 doctors, 2 clinical support workers, and 1 occupational therapist. Of these, 16 (76%) were aware of the project. The average score for level of ease was 2.2, and the most common barrier to success was staffing levels on the ward inhibiting their ability to safely get patients out of bed at mealtimes.
Discussion
These results demonstrate an improvement in three core areas for prevention of HAP: bedhead angles, appropriate use of adult feeding cups over drinking straws; and getting patients out of bed for meals. In the percentage of patients meeting the goals, the respective rises were 23%, 26%, and 21% in these categories.
There were a number of factors aiding the success of this project. First, the widespread acknowledgement that HAP is a serious threat to many patients meant that motivation for success from the senior staff was high. Through education, the repetition of the audits, and each new intervention, 76% of staff became aware of the aims of this project and its significance in their roles on the ward.
In a QIP that relies on a change in human behaviour it is often necessary to facilitate a change in culture and attitude. Throughout the presentations to educate staff the tagline ‘HAP—Habits Aid Prevention’ was repeated to emphasise the importance of changing whole approaches to patient care, in the hope that these practices become second nature.
Lessons learnt
As anticipated there were some minor barriers to success, one of which being that the checklists were time-consuming to complete. These were not well received by staff and were therefore not routinely included for all patients. In the interest of recordkeeping it would be worth looking at reintroducing them in the future in a different format (eg a sticker for the patient notes), or as part of standard admission protocol.
Regarding mouth care and leaflet distribution, this was difficult to assess because it was instigated late in the process a limited result was observed. This could be aided in future by deliberate coordination of events with other divisions of the multidisciplinary team (eg SALT). It would also be beneficial to consider introducing an oral hygiene assessment tool in order to measure the impact of any future changes in this domain.
If time and resources had permitted, it would have been beneficial to know the prevalence of HAP on these wards before and after the project had taken place. This would have added another dimension and allowed direct correlation with how effectively the measures prevented HAP. However, due to the previously mentioned issues with surveillance in NVHAP this was difficult to do. The primary focus of this project was to demonstrate how easily the change in practice could be adopted.
Furthermore, during the research for this project a number of other risk factors for HAP were identified. These were not included in the audits but it is worth noting these other contributing factors, whether preventable or non-preventable. These include, but are not limited to:
Another risk factor that can be addressed on the ward is malnutrition. This has been shown to increase incidence of HAP (Sopena et al, 2014) and can be monitored and prevented with early involvement of dietitians.
Following the first intervention, the wards suffered a busy winter with staffing issues and high patient load, making it difficult to prioritise the HAP project. Despite this, there was a noticeable improvement in preventive care, showing that the interventions were easy to implement even during a busy and short-staffed period.
With regard to sustainability, the complications of hospital-acquired infections are widely acknowledged, therefore this project is significant for the local health system, as well as being relevant across the NHS. Because the project cost was low and many of the measures have already been introduced, its continuation is considered sustainable and therefore advisable.
Conclusions
The results of this project show an improvement in HAP awareness and prevention across the three wards in this QIP. Achievements included 76% staff awareness and clear improvements in three of the measurable preventive strategies. Considering the short time period and minimal cost of this project, the sustainability of these results is promising. The main objective of this QIP was to show that these simple interventions are easy to implement on a busy ward and the results have shown this to be true. The authors hope this will encourage other NHS trusts to consider the simple steps that their nurses and allied healthcare workers can introduce to reduce incidence of HAP in elderly and at-risk patients.