

Nurses returning to practice are a heterogeneous group because they have a variety of backgrounds (self-employed, retired, working in non-nursing health or social care roles, or carers) and academic qualifications (from certificate to PhD level). They had allowed their registration to lapse for a range of reasons, such as caring responsibilities, a life crisis, ill health, relocating abroad or retirement. They are valued for their knowledge and experience, having a love of nursing or midwifery and wanting to make a difference to the lives of patients (Kent, 2015).
This study examined the lived experience of nursing, midwifery and allied health students undertaking a return to practice programme at a university. The first author is programme lead in a university responsible for return-to-practice (RTP) recruitment, and the idea for research was triggered by a returnee comment during a personal tutor session. The returnee had felt criticised for wanting to come back to nursing, and this had a lasting effect on their experience.
The research adopted a qualitative, exploratory approach designed to focus on interpreting returnees' lived experience. Much of the UK RTP literature focuses on programme provision, rather than returnee experience, or uses case studies as part of recruitment drives.
It is important that returnees feel accepted within clinical practice so they can develop professional self-esteem and confidence, which enable a successful return to the workforce (McMurtrie et al, 2014).
Nurses and midwives whose UK registration has lapsed undertake a university-accredited RTP programme approved by the Nursing and Midwifery Council (NMC) to rejoin. Provision of RTP programmes was thought to be patchy and inconsistent across the UK, so HEE scoped the provision and developed a national toolkit that informed programme development and promoted consistency (HEE, 2014). HEE's ‘Come Back to Nursing’ campaign included several phases of development and marketing and has encouraged nurses, midwives and allied health professionals to return.
The NMC (2019) reviewed its RTP standards and introduced a test of competence as an alternative way of regaining registration. This test is like that required by applicants who trained abroad who wish to register in the UK.
With lower attrition rates than 3-year preregistration courses, RTP programmes are cost effective and have boosted the workforce (HEE, 2014).
Context
The numbers of nurses and midwives leaving the profession have been rising at an alarming rate; more than 29 000 nurses or midwives registered in the UK left the register between October 2016 and September 2017 (NMC, 2017). The UK nursing workforce, which was already overstretched, struggled to cope with demand, particularly in specialty areas, and nurses were ‘feeling pressured around morale, standards and retention’ (House of Commons Health Committee (HCHC), 2018: 4). They were 36 000 nursing vacancies in England covering almost every specialty, with agency or bank staff filling up to 33 000 of these; where vacancies were filled, this was mainly in adult nursing (HCHC, 2018).
Nurses primarily left the profession because they felt disillusioned, overworked or undervalued (HCHC, 2018), underpaid and concerned for their own mental wellbeing and the mental wellbeing of their peers (RCN, 2020). Up to one third of all healthcare staff considered leaving their profession between 2019 and 2020 (RCN, 2020).
Leading up to the COVID-19 pandemic, there were around 40 000 nursing vacancies in the NHS in England (Royal College of Nursing (RCN), 2020).
The development of nursing associates and apprenticeships, aimed at addressing the rising number of nurses leaving rather than joining the workforce (Buchan et al, 2019) was the UK's political responses to nursing shortages.
Research approach
This qualitative exploratory research focused on returnees' perceptions of professional practice. It explored returnee experiences and perceptions using focus groups. Research aims and questions directed the scope of the study and determined the methods. The university gave ethical approval.
Aim
The study's aim was ‘to understand the lived experiences of returnees coming back to clinical practice in the UK following a lapse in their professional registration’.
Research questions
The research questions were:
- What do returnees expect their return to practice to be like and how does this compare with their actual experience?
- What are returnees' perceptions about how they are perceived and received by other health professionals and patients in clinical practice during the return-to-practice programme?
- What do returnees view as valuable key personal and professional clinical practice characteristics, if any, about themselves and others and how does this influence their experience?
Participant selection
Returnees were invited to participate using the university's Blackboard Ultra electronic learning platform by a member of staff who was not responsible for their progress. Researchers complied with the General Data Protection Regulation, the Data Protection Act 1998 and university guidance, keeping information confidential and anonymous. Participants gave voluntary informed consent and could opt out at any time without any repercussions.
Sample size and characteristics
Sampling was purposive. Recruitment was from two small RTP cohorts in 2017–2018, and reflected different professional fields (nursing, midwifery and allied health). Twelve returnees took part (two midwives, two occupational therapists, one learning disability nurse and seven adult nurses). The total number of returnees in those cohorts was 28 (16 and 12 in 2017 and 2018, respectively).
Returnees had been out of clinical practice for between 6 months and 20 years. Their professional experience and previous roles varied. Participants had held senior or junior roles before starting the programme and had worked or were working in the NHS, voluntary or private sectors. Others were self-employed in roles unrelated to healthcare. Returnees who participated were supernumerary, as required by the NMC (2019).
Setting
Focus groups were convened in a university. A comfortable setting was provided at a time convenient regarding the returnees' timetable to minimise disruption to learning. Only researchers and returnees were present at the focus groups.
Data collection
Three focus groups took place lasting between 45–60 minutes, engaging returnees at different stages of their clinical placement. These were facilitated by a member of staff not responsible for determining returnee progress and audiorecorded. Data were anonymised and no local organisation, staff, returnees or patients were identified.
On-the-spot member checking took place to ensure data collected reflected returnee voices (Birt et al, 2016). This confirmed accuracy and clarified the meaning of what was being said or implied.
A focus group schedule, pilot tested for usability, guided the data collection. This had several themes and included open, probing questions (Box 1). Returnees were encouraged to tell their stories; they shared experiences spontaneously and ‘bounced off each other’ (Tausch and Menold, 2016).
Box 1.Focus group schedule and discussion questionsGoing back into clinical practice
- What were your expectations of returning to clinical nursing practice?
- What happened on your first day back?
- What were your initial impressions?
- How do you think your were received by other nurses during the programme and in clinical practice?
Identifying changes
- What do you think has changed about the patients since you left nursing practice?
- What do you think has changed about the staff since you left nursing?
- What do you like most about going back into clinical practice (nursing)?
- What concerned you the most about going back into clinical practice (nursing)?
Communication
- What kinds of things did you talk about with your practice supervisor/practice assessor?
- What information have you found the most helpful?
Perceptions and values
- How do you think you were perceived by other nurses during the programme and in clinical practice?
- What about patients' perceptions of you as a student?
- What do you think was valued most about you by other team members?
- What do you think was valued most about you by the patients?
- What do you value about yourself?
- What has been as a surprise?
- Thinking back to your initial expectations, how did these compare with your actual experiences?
Probing questions
- Tell me a little more about that.
- Is there anything else you would like to add?
- Tell me more about how that makes you feel
- Can anyone else add their thoughts to that question?
Clarifying questions
- I want to make sure I have a clear picture of what you are saying—can you explain it again?
- Can you give me an example of what you mean?
- Does everyone think the same?
Data analysis
Focus groups were recorded and transcribed, and data were analysed manually using thematic analysis (Green and Thorogood, 2014). This four-stage analysis, accessible to the researchers, offered flexibility (Nowell et al, 2017). Analysis, coding of transcripts and theme identification had an audit trail for transparency.
To become familiar with the data (stage 1), two researchers independently listened to recordings, took notes, gained first impressions and compared for similarities and differences. Each transcript was read individually several times, and the researchers returned to and listened to the recordings to rediscover sounds, expressions and intimations of returnee voices. The researchers independently annotated each transcript, having agreed what evidence they were looking for, such as coping strategies in clinical practice. This determined initial codes and highlighted key themes, which were labelled using a coded numbering system (stage 2). Across the three transcripts, 153 separate codes were identified between the two researchers.
An iterative comparison then took place to reduce the number of codes. This resulted in 27 emerging categories within the data set (stage 3). Each category was reordered and colour coded (stage 4) (Figure 1).
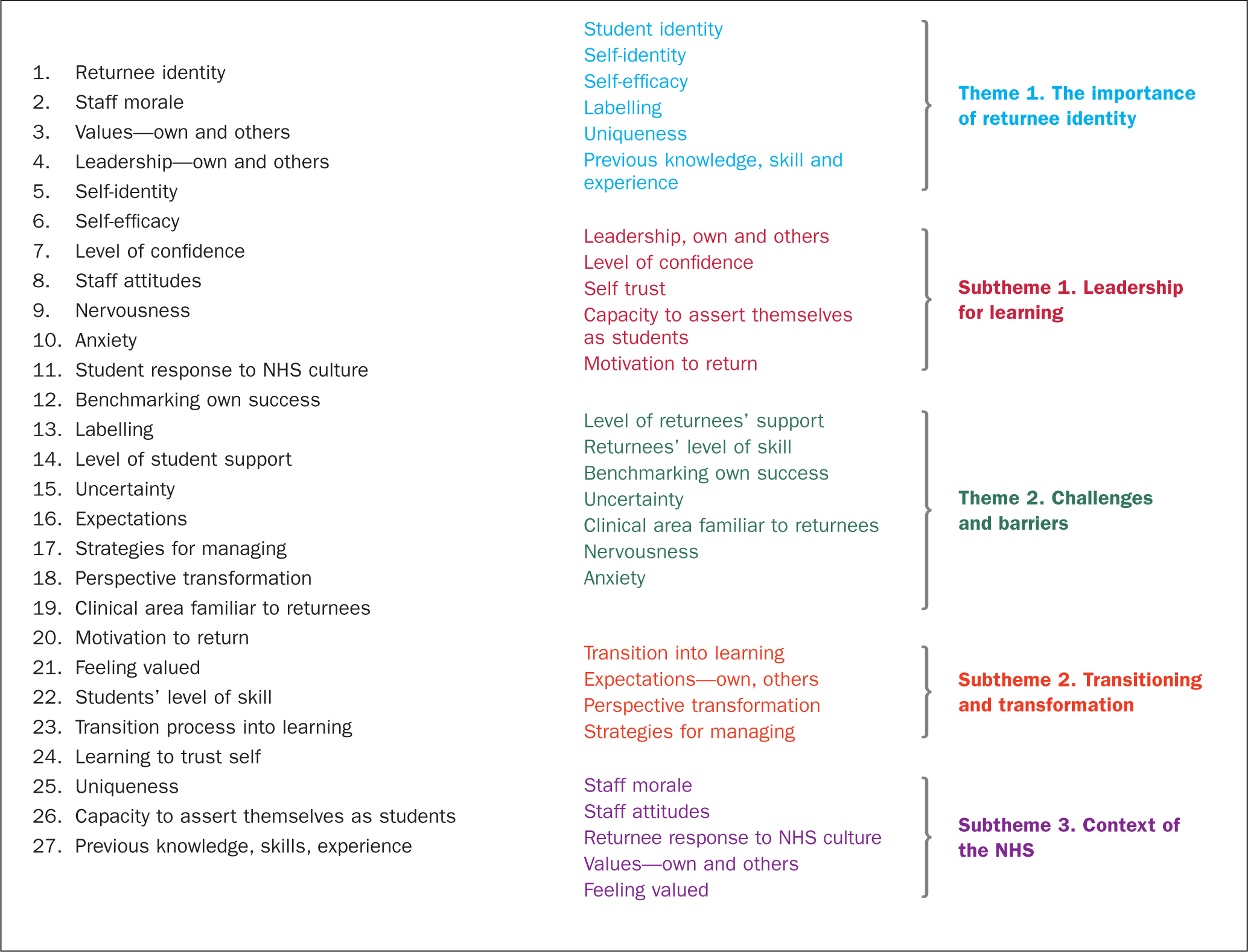 Figure 1. Thematic analysis—codes, categories and themes (Green and Thorogood, 2014)
Figure 1. Thematic analysis—codes, categories and themes (Green and Thorogood, 2014)
Overall, two key themes and three subthemes emerged from the data analysis:
- Theme 1: the importance of returnee identity
- Theme 2: challenges and barriers to learning
- Subthemes: leadership for learning; transitioning to transformation; and context of the NHS.
Findings
Theme 1. The importance of returnee identity
One of the clearest and strongest emergent themes was the importance of identity, which was expressed as role ambiguity. Some returnees articulated concern about how they were perceived by other healthcare staff, patients and colleagues because of their previous role, position, experience and/or length of absence from practice.
They were concerned about how their previous registered status affected their returnee journey in clinical practice. Initially, most returnees were cautious, nervous and lacked confidence.
One returnee was concerned about how she would be received, having been in a senior position:
‘I was very nervous about how I would be received. I guess having left as a very senior nurse and coming back as a student … and how that would be perceived by the staff was the main thing that concerned me.’
Returnee, Focus Group 2
All returnees expressed that it was common for clinical staff, patients and relatives not to fully understand what role they had. Returnees repeatedly had to introduce themselves and explain their role to the point where they provided a history of what led to up being a returnee and included why they were there:
‘I have been asked a lot of times … “What are you?”’
Returnee, Focus Group 3
Ambiguity of returnee identity presented a challenge to returnees' way of thinking about themselves and others' views of them. On one hand, they had experienced life as a qualified nurse, midwife or allied health professional while, on the other, they had supernumerary status. This scenario generated uncertainty as to their persona:
‘It's such a challenge because they don't know who we are when we walk on the ward, they don't know what our experiences are … they don't know what box to put us in.’
Returnee, Focus Group 1
Returnees felt that ambiguity and identity influenced the relationship they developed with their practice supervisor (PS) and practice assessor (PA) (NMC, 2018) because they added a layer of complexity when it came to assessment. Returnees were uncertain about their self-expectations and the expectations of the PS/PA. They established ways of managing this to aid the learning experience and provide a level of self-protection. Some felt protected by their student uniform:
‘I feel wearing white is a … safeguard … It means expectations are not too high.’
Returnee, Focus Group 2
‘I do like it [the white uniform] … it is like a security blanket.’
Returnee, Focus Group 2
For some returnees, the knowledge, skills and experience known to them yet unknown to their PS/PA made an awkward juxtaposition. They recognised their student status, the need to progress and a desire not to alienate the PS/PA or undermine their relationship with them:
‘I am a student, but there is a bit in the middle. There is a bit that nobody knows about me. We are all different and the mentor is struggling with that unknown entity … I think it is a very tricky place to be as a student because you don't know what people's expectations are for yourself and you are a threat to other people.’
Returnee, Focus Group 2
This juxtaposition had the potential to be a barrier or challenge if not managed correctly.
Theme 2. Challenges and barriers to learning
Returnees raised and recognised emotional challenges faced in clinical practice. This included worry and anxiety about performance. They described themselves as ‘embarrassed’ ‘vulnerable’, ‘scared’ or ‘terrified’. They imagined the job had greatly changed since they last practised as a nurse, midwife or allied health professional and that their knowledge and skills were inadequate to fulfil the role they had once been competent to do:
‘I was I worried that I would have completely forgotten everything and become so deskilled in all the practical side that I wouldn't be able to do anything in the beginning.’
Returnee, Focus Group 3
One returnee was negatively questioned by a member of clinical staff about their motivation to come back to the profession. They interpreted this as disillusion with working in the NHS:
‘I had one very experienced nurse saying, “we are all trying to get out and you are coming back—you are an absolute fool”.’
Returnee, Focus Group 2
However, this kind of response did not appear to deter returnees and they articulated their own motivations for why they wanted to return:
‘My journey is my journey and yours is yours. I left for reasons and am coming back for reasons because they are mine and this is what I've chosen to do.’
Returnee, Focus Group 1
Clinical staff embraced returnees’ motivations for joining the programme, provided positive feedback and valued returnee contributions. They valued their ability to engage in the learning experience and use transferable knowledge and skills in clinical practice. When asked directly by the researcher: ‘What was valued most about you as a returnee by other team members?’ returnees responded:
‘Coming with a little experience and knowledge and you are not hard work [in comparison to other students].’
Returnee, Focus Group 2
‘Enthusiasm … we are more proactive [than other students].’
Returnee, Focus Group 3
Subtheme 1. Leadership for learning
Returnees valued placements that encouraged them to take the lead in managing and organising the learning experience. They described this as successful when it suited their individual learning style and level of confidence, where they were in control of the pace of the learning plan and could articulate their own learning needs.
Some returnees were more cautious than others in their management of the learning environment:
‘When I went to the ward, I was expecting the worst because I knew everything has changed, but … it has been lovely. I said to my mentor “I don't want to do anything at all, I just want to observe for the first two weeks”.’
Returnee, Focus Group 3
It was important for returnees, as part of their learning journey, to be able to tell a PS/PS what knowledge and skills they would like to acquire, develop or already have to function in clinical practice, and to openly articulate their learning plans to their PS and PA. However, this presented a further juxtaposition between the knowledge and skills they had—ie the practicalities of nursing, midwifery or allied health profession work—and how to define these within the context of their individual requirements:
‘You have the knowledge and skills in relation to how to go on and it's really hard to sort of define the return-to-practice role and I have found, personally, that it has been very much a case of leading my own learning.’
Returnee, Focus Group 3
Where clinical staff had previous positive experiences of supporting returnees, this influenced the learning experience in a positive way. They were more familiar with returnees and RTP programme requirements. Familiarity and understanding were significant because they appeared to remove a layer of uncertainty felt by both returnees and their PS/PA. This was especially so if those familiar with RTP were in a leadership position and consequently influenced other clinical staff:
‘The [ward] sister … makes a massive difference, she really has been very accommodating. She has experience of return-to-practice students and that has made a huge difference.’
Returnee, Focus Group 3
Conversely, the learning experience was negatively affected if previous returnees had left before completion, struggled to express a clear rationale for returning or were unable to demonstrate a level of practice commensurate with professional body requirements and the expectations of clinical staff and academic programmes. Rather than a layer of uncertainty being removed, a layer of uncertainty was added:
‘My PS, she had some bad experiences with return-to-practice students. Some hadn't finished and some she didn't know why they were coming back at all … her first impression wasn't good, but she was very nice, and she chatted to me a lot and she was great in the end—but her first impression wasn't good of return-to-practice students.’
Returnee, Focus Group 1
Subtheme 2. Transitioning and transformation
Returnee transformation was felt to be gradual and returnees were surprised at the pace at which they progressed and transitioned towards re-registration during their studentship.
Where returnees were on placement in areas of clinical practice that were familiar to them, transition was smoother.
They considered the demonstration of knowledge and skills as a personal benchmark:
‘Once I got in, it's as if I've never been away… Trusting my own clinical knowledge and clinical skills … I am not as far off the mark as I thought I was going to be.’
Returnee, Focus Group 1
Clinical staff 's recognition and support of returnees' positive transition towards re-registration was important. This increased returnees' confidence, which then enabled their confidence to grow further.
Returnees articulated the positive contribution they made during their learning journey:
‘As the placement went on, I actually realised that some of the [knowledge and skills] I was bringing in were far superior.’
Returnee, Focus Group 2
At the beginning of the placement, some returnees perceived themselves as having equal status to third-year preregistration students. By the end of the placement, returnees felt they had transitioned to the same level as the PA and PS—returnee to peer. They were confident enough to provide feedback to their PS/PA as part of a two-way learning process. However, this was linked more to the perception that these staff members received little positive feedback from other sources, and returnees desired to fill this gap:
‘I did find myself giving positive … and constructive feedback to the PS because I felt that was the only route they got it … in order to get the best … you need to be equal with them.’
Returnee, Focus Group 1
Returnees recognised the positive contribution they made and the importance of a two-way learning process where they could give back to their PS:
‘Towards the end … my PS said she had learned so much from me.’
Returnee, Focus Group 1
Subtheme 3. Context of the NHS
Several returnees discussed how the current political climate influenced the mood of some clinical staff. Returnees perceived that clinical staff found negative portrayal of the NHS difficult to deal with. Returnees emphasised that praise and encouragement for clinical teams from leaders, patients and relatives were important for staff morale.
They had reflected on their experiences of coming back and recognising the importance of positive feedback for all NHS staff:
‘They were taking it really personally … they need to hear that they are good at their job’’
Returnee, Focus Group 1
Discussion
The findings of this research illuminated returnees' experience of their journey back to nursing, midwifery or allied health professions and generated several areas for discussion (Figure 1).
Impact of returnee identity
Returnee identity appeared to be more complex than first thought and was important to returnees. Health professional identity is diverse and is required to be well defined to demonstrate worth (Arreciado Marañón and Isla Pera, 2015).
However, both returnees and clinical staff had difficulty defining professional identity as it related to returnees because of role ambiguity. Returnees had been socialised to develop a professional identity as students and later as a member of a professional workforce (Arreciado Marañón and Isla Pera, 2015).
Identity mattered to all the returnees taking part in the research. It was often the first thing raised when discussing experiences of returning. There was familiarity with the meaning of the word student in clinical practice, although this did not always develop into understanding what it meant to be a returnee. Returnees viewed their identity through their own and other's perceptions of them as they navigated their way back to the profession that many had left.
From the returnee perspective, identity focused on ensuring that patients, relatives and staff, particularly the PS and PA, understood who they were and what they had to offer. The PS/PA role was critical in helping returnees to transition during the programme (Draper et al, 2014). When previous professional experience was explored, exposed and understood, as it merged with the new experience, returnees were enabled to meet NMC requirements for the programme. This previously undisclosed background was described as the ‘bit in the middle that nobody knows’. As returnees often felt nervous, they wanted an individual approach to the learning experience because those ‘middle bits’ were individual to them.
Some felt safeguarded by their student uniform, which prevented rapid exposure to the complexities of practice and higher expectations of others before they felt ready. Others were keen to stand out from the crowd and have their previous status as being registered health professionals recognised as early as possible albeit within the confines of supernumerary status.
Returnee learning needs
Returnees and clinical staff recognised their learning needs were different from those of other students. However, this was more about what they were not than what they were. They were not third-year preregistration students, new to professional practice, nor re-registered—they were somewhere in between. Being in this position was significant because it shifted their identify and role to a place where a pattern for learning was less recognised; there was a mismatch between information readily known (what and who is this returnee) and seen (a supernumerary student in a white uniform) and that which is hidden from view (previous professional knowledge, skills and experience).
Returnees' knowledge, skills and competence reflected a uniqueness described in the findings as ‘the bit in the middle that nobody knows’, as they had not disclosed this information at the time. Some returnees described being ‘overlooked’ by both staff and patients because of returnee student status, the white uniform and a lack of understanding of their role. Others perceived clinical staff were intimidated by their previous senior healthcare roles. Perhaps this blurring of boundaries caused returnees to be reluctant or find it difficult to articulate exactly who and what they were in terms of current and previous experience.
Returnees' perceptions of success for transition and transformation
Returnees did not perceive the length of time away from clinical practice as defining the parameters for success and return to the profession they had once loved.
Some returnees were anxious about appearing inept and inadequate, fearing that clinical staff and patients would be critical of their performance. Those returnees held back, preferring to feel safe without quick exposure in practice. Others expressed the need for a uniform that differentiated them from preregistration students so they could stand out and be noticed.
Once returnees were able to interpret, expose, separate or integrate their current role with their previous professional knowledge and experience, the ‘bit in the middle’ became more transparent and this benefited the learning journey. This happened when the returnee, with the PS/PA, gained the capacity to disclose what had been hidden.
As the learning journey of returnees is plotted (Figure 2), the role of the PA/PS and returnee are established, and the identity of the returnee becomes more tangible. This can be likened to a perspective transformation (Mezirow, 1978), where returnees viewed themselves as different because they demonstrated the knowledge and skills required to be equal to their registered peers.
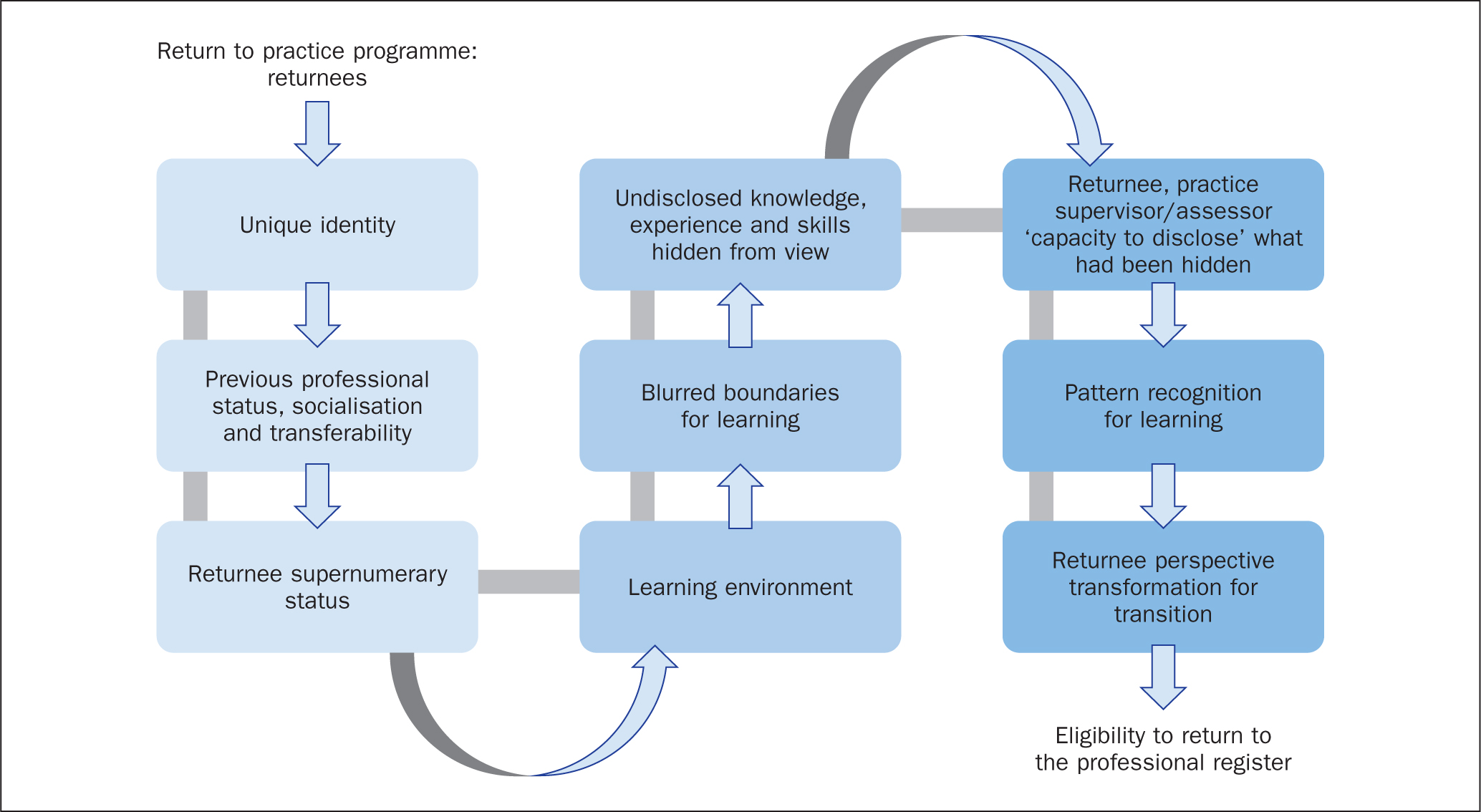 Figure 2. The learning journey and professional identity
Figure 2. The learning journey and professional identity
Where returnees were able to lead the learning process, they gained valuable learning opportunities. They used their own experience of supporting past learners and took advantage of individual learning experiences in a way they felt they would not be able to once back on the professional register. Feelings of belonging within the team helped them to recognise their contribution to the workplace often with a freshness, despite their initial trepidation.
Returnees not able to transition successfully felt less integrated into the team and less confident about continuing.
Returnee perspectives on praise
Returnees acknowledged that praise was important to improve retention, job satisfaction and the NHS working environment. Praise is a simple, cost-effective mechanism for reward and recognition that managers can give staff (Sveinsdóttir et al, 2015).
Returnees were empathetic and expressed concern about their professional colleagues. They perceived them as receiving negative feedback when something had gone wrong but not praise when something had gone well and for good practice.
When staff commented negatively about people returning to practice and their reasons for doing this, returnees linked this to staff morale resulting from the broader impact of the existing culture of leadership and political climate within the NHS. While this was an assumption on the part of the returnees, it is supported by a reduction in the numbers of nurses and the rationale for them leaving the workforce (HCHC, 2018; RCN, 2020).
Limitations
This was a small-scale, qualitative research study, limited by the number of participants. Researchers had access only to returnees in their own higher education institution so findings were limited to a specific region and may not apply to experiences elsewhere. One method was used; further research could include semistructured interviews in addition to focus groups.
Conclusion
This research highlighted the experiences of returnees on an RTP programme; there is a lack of similar research looking at this. It focused on interpreting returnee perceptions of how they were received and perceived in clinical practice.
Previous knowledge, skills and experience were initially hidden and hard to explain, and this was further complicated by the ambiguous nature of returnee professional identity. When boundaries around identity were blurred, this affected the process and speed of transition from returnee to successful completion. Where returnees were placed in areas of clinical practice that were familiar to them, transition was smoother.
Where previous experience of RTP learners in a clinical setting had been negative, this could interrupt the learning process and exposure of the knowledge and skills required for success.
Success was dependent on two factors; the propensity of the returnee to expose their worth and navigate the learning journey; and the ability of the PS and PA to transverse blurred boundaries to meet returnee needs.
In addition, returnees' identified that clinical staff needed to be recognised and praised more readily where there was consistent good practice.
KEY POINTS
- Returnees' perceptions about their identity was a key theme during the programme. The effect of this varied
- Several barriers and challenges to re-establishing clinical knowledge, skills and experience existed for returnees. How they managed this depended on capacity to lead the learning experience.
- When they perceived that NHS clinical staff were not given regular praise, returnees were empathetic
- Transitioning was individual; it varied in length and depended on the learning environment
CPD reflective questions
- What barriers and challenges that affect returnees' transition exist in your area and how could these be addressed?
- Why is it important for practice supervisors and practice assessors to understand and facilitate returnees' individual learning needs?
- How would you describe the returnees' experience here and how does this equate with your own learning style, facilitation of learners and experience?