

All patients with advanced, progressive and life-limiting illness should receive the best possible care throughout their palliative diagnosis and into death, regardless of where they live and die. There is a plethora of national guidance that supports the fundamental requirement for all staff to have the knowledge and skills to competently deliver high-quality palliative and end-of-life care (EoLC) regardless of where the patient is cared for (Department of Health (DH), 2008; Leadership Alliance for the Care of Dying People 2014; Healthcare Quality Improvement Partnership, 2019; National Palliative and End of Life Care Partnership, 2021). However, Cicely Saunders International (2021) identified that only 10% of nurses felt prepared to deliver good palliative and EoLC. One reason for this was lack of education.
Education is key to delivering the Ambitions for Palliative and End-of-Life Care national framework (National Palliative and End of Life Care Partnership, 2021), which is a national document designed for local implementation to improve EoLC. It is recommended that education must be delivered to all staff groups and at all levels (DH, 2008). Despite the education of staff in all areas being a significant task for NHS providers (Wee, 2016), it is acknowledged that palliative and EoLC education significantly increases staff knowledge and improvements in patient care (Lehto et al, 2017; White et al, 2019). Therefore, it is essential that all healthcare staff can access good palliative and EoLC education to improve patient care.
An ageing population and increased life expectancy for palliative patients will continue to result in higher demands on palliative care services in all settings (Williams et al, 2010). It was predicted in 2017 that half a million people would require palliative care by 2040 (Das, 2021), yet this was reached in 2020 due to the COVID-19 pandemic. The increasingly complex needs of palliative patients (Frey et al, 2019) further necessitate the need for all staff to be equipped to deliver high-quality palliative and EoLC. Therefore, the trust in which this service evaluation took place has a team of EoLC facilitators who deliver a wide range of palliative and EoLC education to all trust, care home and domiciliary care staff. The objective is that palliative and EoLC is improved for all patients in the geographical area of the trust, regardless of where patients live and die. The trust is a mediumsized NHS trust in the north-east of England.
The education evaluated consisted of two 1-day courses, a 6-week course and a 4-day course. The 1-day courses are End-of-life Care Level 2, aimed at non-registered staff such as healthcare assistants, porters, ward clerks and care home staff, and End-of-life Care Level 3, aimed at registered staff such as nurses, allied health professionals and doctors. Both courses cover topics such as national, regional and local guidance, the fundamentals of palliative and EoLC, holistic care, advance care planning and symptom control, with a level of detail aimed appropriately at the staff attending. Following attendance at Level 3, registered staff can attend the 6-week Palliative Care Foundation Course, which covers palliative and EoLC in much more detail. Staff are required to complete a workbook and present a case study in week 6 to successfully complete the course. Following successful completion of the foundation course, registered staff can attend the Palliative Care Advanced Course. This course includes guest speakers on palliative and EoLC in specialist areas and goes into more detail about symptom control. There is an assessment on day 4, which needs to be passed to complete the course. The foundation course and advanced course are accredited by an external awarding professional body.
The EoLC facilitators lead and deliver the majority of the palliative and EoLC education in the trust, with some support from the trust's palliative care team, consisting of community and hospital palliative care nurses. Currently, attendance at all courses is optional and staff voluntarily book onto the education sessions via the learning and development team or through the electronic staff record portal.
Education is evaluated immediately after delivery to assess the quality of the content and delivery. However, staff confidence levels in delivering palliative and EoLC, and how education may improve patient care are not currently assessed. This is important as evaluation of palliative and EoLC education should not only include application to practice but should extend beyond the point of delivery (Leadership Alliance for the Care of Dying People, 2014).
Aims
The purpose of this study was to evaluate staff confidence levels in delivering palliative and EoLC to patients following attendance at trust education. The secondary purpose was to explore whether staff that perceive patient care has been enhanced through course attendance.
Method
Design
Primary data collected in health care can provide secondary data to support service evaluation and research (Dunn et al, 2015; Evans, 2018; Hutchings et al, 2020). Secondary data were used for this study in the form of staff surveys as this was relevant existing and accessible data. The purpose of the survey was to collect data on the staff 's perceived confidence levels pre- and post-education because this was something not previously assessed. The survey responses provided quantitative data around staff confidence levels and qualitative data in the form of free-text comments. This mixed-methods, pragmatist approach supported the purpose of the evaluation to establish ‘what works best’ in educational practice, and to increase validity through triangulation of data (Johnston, 2014). The survey was completed using Microsoft Forms, enabling participants to complete them electronically. The survey was sent to all staff who had attended End-of-Life Care Level 2, End-of-Life Care Level 3, Palliative Care Foundation Course, and Palliative Care Advanced Course between 1 January and 31 December 2022. All staff were chosen because they had attended the courses being evaluated. There were no exclusion criteria.
Data collection
Surveys (Box 1) were sent via an email introducing the survey and the rationale behind it. A total of 238 surveys were sent with a 3-week deadline. The survey looked at the link between staff confidence levels and staff perceived improvement in patient care following attendance at the courses, which evidenced construct validity because it measured what it was intended to measure (Smith et al, 2022).
Palliative and end-of-life care education evaluation survey questions
The questionnaire was sent to all registered and non-registered staff who attended trust palliative and end-of-life care education in 2022, to ascertain the effects of the courses attended on staff confidence and patient care
The survey response rate was 31 (13%). There was a 4-day strike by junior doctors during this time, which may have impacted on the survey response rate because staff were busy covering for the absence of junior doctors.
Data analysis
Quantitative data analysis examines numerical data to confirm measurements and identify trends and relationships (Watson, 2015). As the survey was completed via Microsoft Forms, pie charts were automatically generated from the quantitative data. However, these data were then converted to bar charts for ease of reading and for data analysis.
Qualitative data were coded using thematic analysis, which is a flexible and accessible method that allows insight into themes within the data (Braun and Clarke, 2012). Re-reading and checking the data provided a comprehensive and careful analysis, which helped to reduce bias (Gibbs, 2018). Although qualitative research software is often used to code qualitative data (Sutton and Austin, 2015), due to the small-scale nature of this study coding was performed manually. However, a second opinion was requested from a work colleague with experience of data analysis to establish the credibility of the coding, thus increasing the trustworthiness and rigour of the study (Sutton and Austin, 2015).
Ethical considerations
The service evaluation was granted ethical approval from Teesside University ethics committee and the trust. As the first author works in clinical education, it is important to recognise potential bias in this study. To mitigate this, an audit trail of the study was recorded to examine the study process. An audit trail helps to ensure that the authors acted with integrity (British Psychological Society, 2021), evidencing honesty and transparency (Gibbs, 2018). This reflexivity enhances the trustworthiness of a study (Jolley 2020) and is integral to qualitative work (Jootun et al, 2009).
Quantitative findings
Course attendance
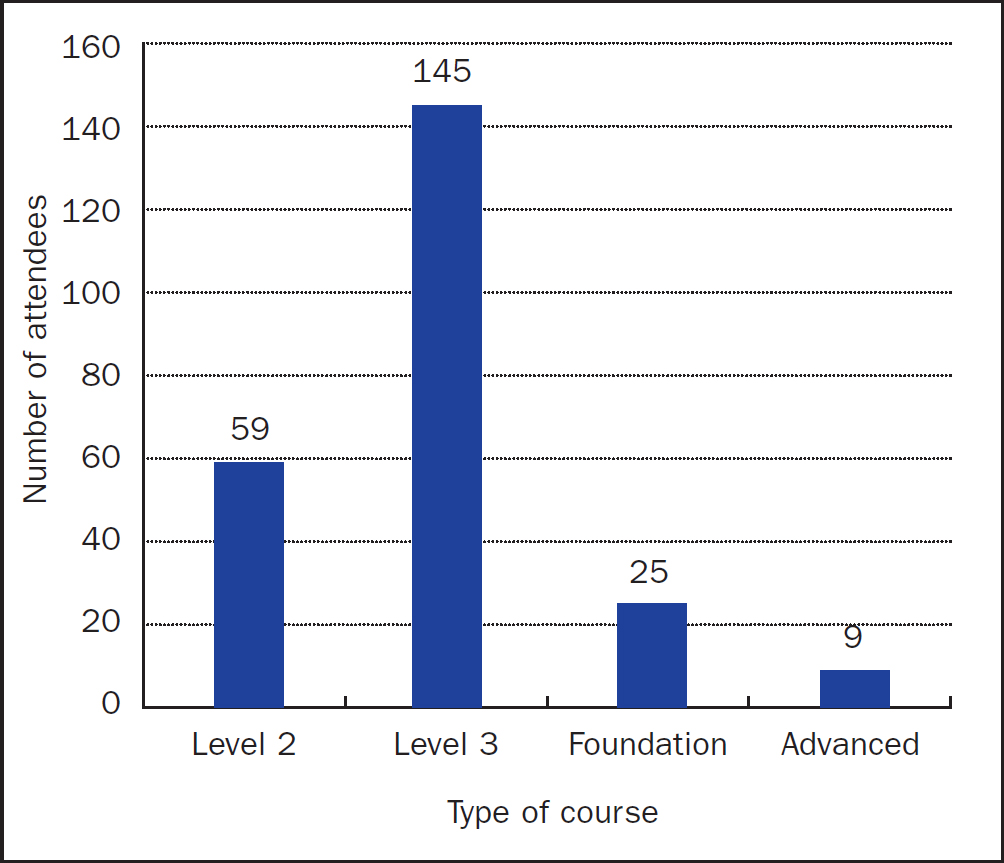
Figure 1 presents a breakdown the courses the participants had attended. The course most attended was End-of-life-Care Level 3 (61%) followed by End-of-life-Care Level 2 (25%). This may be because of the frequency of course delivery with levels 2 and 3 being available monthly, whereas the Foundation and Advanced Course are only delivered twice a year. Consequently, 204 (86%) of the surveys sent out were to staff who had attended the one-day courses.
Relevance of palliative and EoLC education
The majority of participants were staff nurses with others including healthcare assistants and allied healthcare professionals. Specific demographic details have been omitted to maintain participant confidentiality.
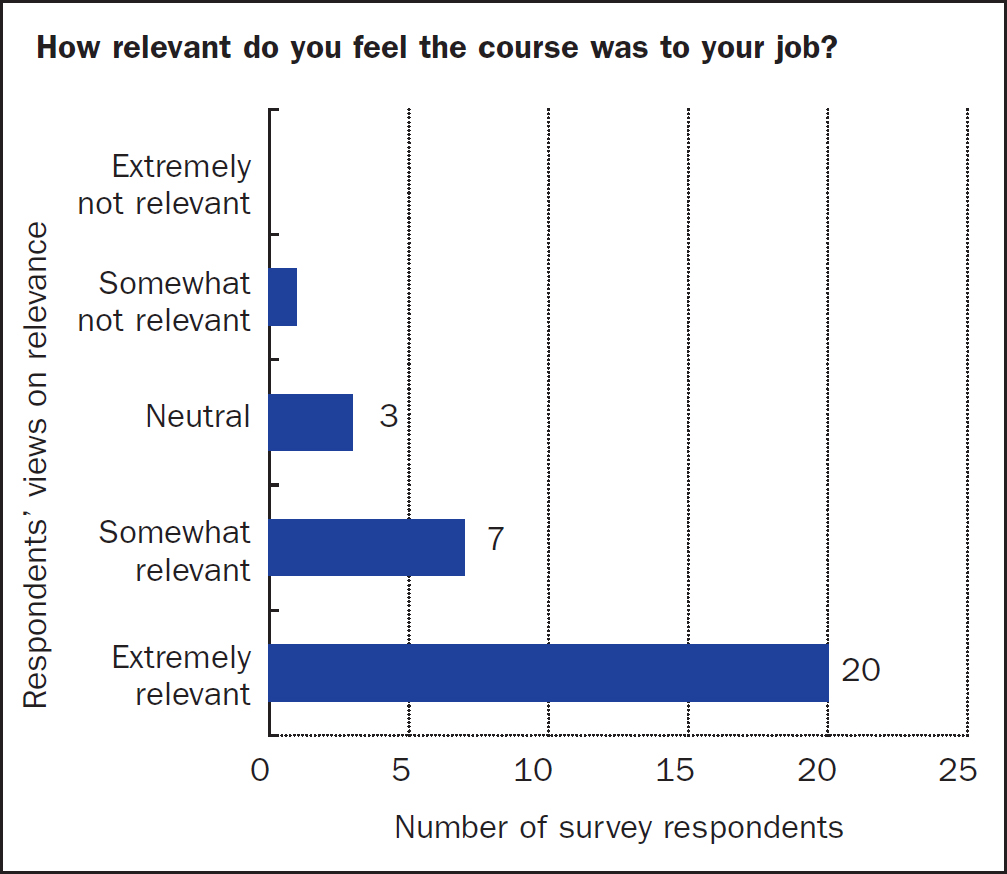
When asked how relevant staff thought the course was to their job, 20 (65%) replied ‘extremely’ and 7 (23%) ‘somewhat’ (Figure 2). Only one person reported that they thought the education was ‘somewhat not’ relevant to their role.
Staff confidence levels
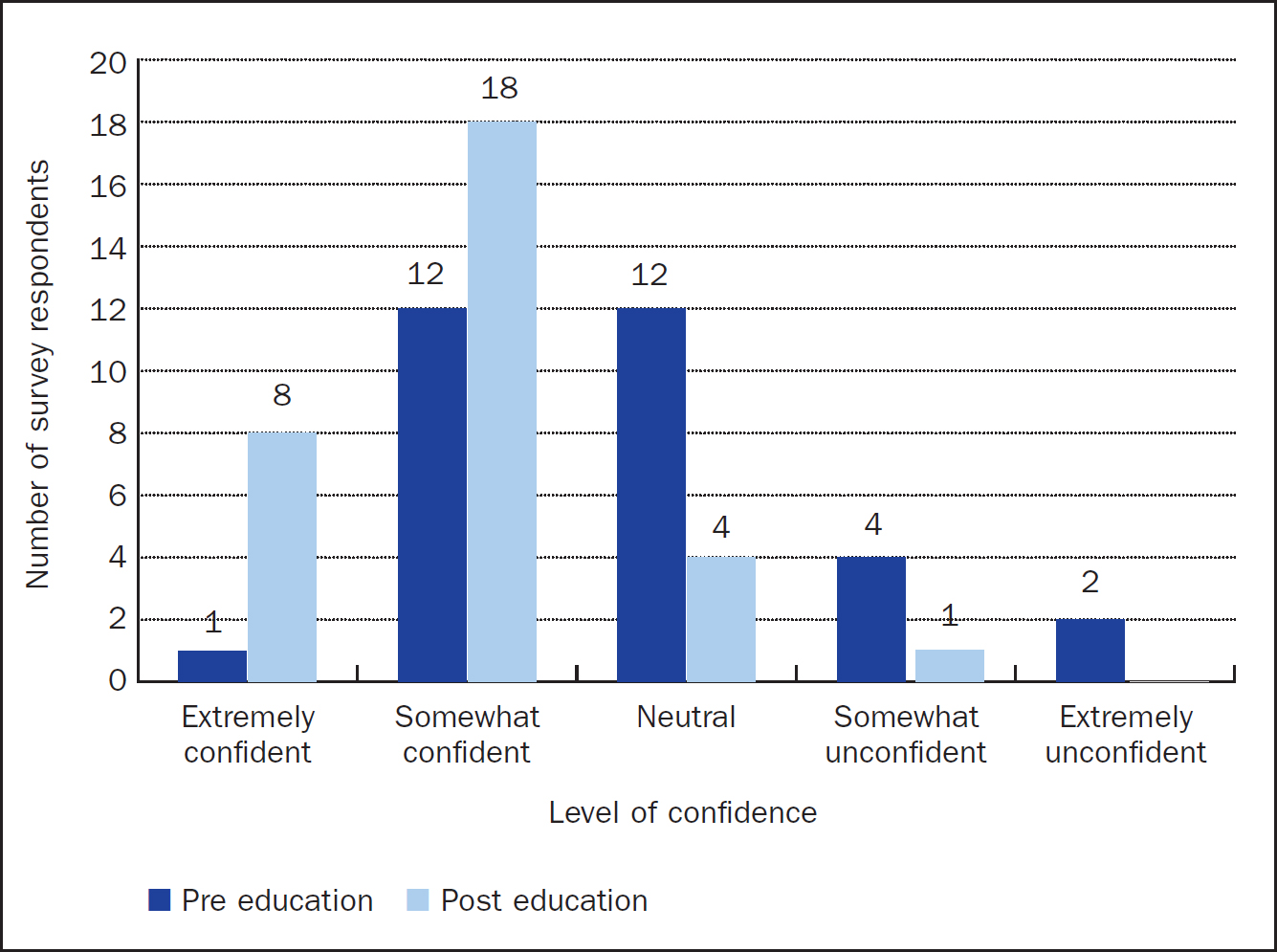
When asked how confident staff had been in delivering palliative and EoLC before they attended the course, 12 (39%) responded ‘somewhat’, which increased to 18 (58%) after they had attended education (Figure 3). This is an increase of 19% in absolute terms. Only one person (3%) reported they were ‘extremely confident’ pre-education. However, following education, 8 (26%) participants reported they felt ‘extremely confident’. This is an increase of 23% in absolute terms. Six staff members (19%) responded ‘somewhat unconfident’ or ‘extremely unconfident’ prior to education, which reduced to just one person (3%) following course attendance. This is a reduction in staff feeling unconfident of 16% in absolute terms.
Qualitative findings
Five main themes were identified, all of which relate to aspects of the delivery of holistic care and advance care planning within palliative and EoLC on which the courses are based. The themes were:
Holistic care encompasses the total care of a person, incorporating the physical, psychological, spiritual and social aspects (Zamanzadeh et al, 2015). Advance care planning is a phrase used to describe conversations that provide patients with the opportunity to discuss their wishes and preferences with their families and carers so they can plan their future care and support while they have the capacity to do so (National Institute for Health and Care Excellence (NICE), 2019). Consequently, the themes identified are intricately linked.
Symptom control
Staff reported higher levels of confidence in managing patients’ symptoms and knowledge of medication required in EoLC. They perceived that patient care was improved due to this increased knowledge. One participant said:
‘Being able to request specific medications that a patient needed and the junior doctor was not aware of due to being mainly used in palliative care allowed better and timely treatment.’
Effective symptom control for patients is pivotal to delivering good palliative and EoLC because it improves the quality of life for patients (National Palliative and End of Life Care Partnership, 2021). Participants reported that they felt equipped with the knowledge and confidence to talk to medical staff about symptom control. This emphasises the importance of education in ensuring the delivery of high-quality care (Cicely Saunders International, 2021). It also highlights a knowledge gap among some junior doctors, which needs to be addressed in accordance with national guidance (Leadership Alliance for the Care of Dying People, 2014).
Psychological support
Supporting patients and families psychologically was mentioned by several participants. Staff reported that they felt more able to emotionally support patients and families. When asked about confidence levels post-education, one participant answered:
‘This course helped me to feel more confident in dealing with all the emotions around this difficult time.’
The education delivered within the trust focuses on holistic care and its significance in palliative and EoLC, to which psychological care is integral. The Ambitions for Palliative and End of Life Care framework (National Palliative and End of Life Care Partnership, 2021) identifies that all patients should be treated as individuals with holistic care at the core. Therefore, symptom control and psychological support are inextricably linked themes because they are both elements of holistic care.
Holistic care
Holistic care was referred to by several participants. In answer to how patient care had improved following education, one participant commented that it allowed:
‘[a] further in-depth holistic care approach.’
This is crucial learning because holistic care is integral to good palliative and EoLC (National Palliative and End of Life Care Partnership, 2021). Therefore, all trust palliative and EoLC education emphasises the importance of holistic care. However, it is significant that staff have integrated this learning into practice because it evidences the impact of education on patient care. This reflects the findings of a former study, which found that palliative care education significantly increased staff knowledge and improvements in patient care (White et al, 2019). This is important because it is essential that all staff are competent to deliver high-quality EoLC (DH, 2008; Healthcare Quality Improvement Partnership, 2019) and are ‘prepared to care’ (National Palliative and End of Life Care Partnership, 2021).
Compassionate care was also mentioned when staff were responding to open-ended questions regarding the impact of education on staff confidence levels and patient care. One participant stated:
‘I'm confident that I can deliver effective and compassionate care to my patients who approach EoL and can support their families through the difficult times.’
The Ambitions for Palliative and End of Life Care framework (National Palliative and End of Life Care Partnership, 2021) and the Leadership Alliance for the Care of Dying People (2014) have highlighted the importance of staff delivering compassionate and holistic care to patients.
Patient advocacy
In response to confidence levels post-education, another theme identified was patient advocacy. One participant noted:
‘I feel more confident in challenging the medical team when I think a patient is nearing the end of their life. Unfortunately, my experience in the past is that I haven't always been listened to and the patient hasn't been assessed quickly enough to initiate EoL care.’
Lack of medical recognition that a patient was dying was noted by another respondent, which highlights a training need for medical staff. These findings are important because it is crucial that all staff feel confident to advocate for their patients. Maximising comfort and wellbeing for patients and ensuring good symptom control are central to delivering good EoLC (National Palliative and End of Life Care Partnership, 2021). If staff feel confident to trust their instincts based on experience and education and advocate for their patients, patients will receive better care by having their needs identified and met.
Advance care planning
Advance care planning conversations were mentioned by several participants. One participant described how patient care had been improved because they had attended the education provided:
‘Feeling able to be open and honest so my patients’ wishes could be discussed with their families and carers … it opened up conversations that may have been avoided.’
This highlights substantial learning about the significance that advance care planning has on patient care. Had this opportunity been missed by the staff, the patient's wishes may not have been heard and acted upon. In total, 75% of the respondents who felt more confident having these conversations had attended the Foundation Course. This course provides in-depth learning about the importance of advance care planning discussions with patients and families. This is an essential element of palliative and EoLC as it ensures patients are central to decisions about their care. Open, honest and timely conversations with patients and families about what matters most to them ensures that patients receive individualised holistic care (Leadership Alliance for the Care of Dying People, 2014; National Palliative and End of Life Care Partnership, 2021). Education is key to achieving this (Cicely Saunders International, 2021), as this study illustrates.
Discussion
This study demonstrates that trust palliative and EoLC education increases staff confidence levels in delivering care to patients. It also reveals that most staff think that palliative and EoLC education is important to their role. These results echo an earlier study looking at medical students’ views on the significance of palliative and EoLC education (Pieters et al, 2019). In this current study, 65% of staff reported that the education was ‘extremely relevant’, with only one person reporting it as ‘somewhat not relevant’. This may be due to the specialty in which the participant worked, as the demographic data indicated a mix, including acute-based care.
When asked for any other comments, the main theme arising was the perceived value of the education. The value of education was referred to frequently throughout the three open-ended questions. This highlights a significant appreciation of the education delivered. Participants reported increased confidence levels in providing holistic care to patients. Having advance care planning discussions and being an advocate for patients were also highlighted. This is crucial to delivering good palliative and EoLC (Cicely Saunders International, 2021; Care Quality Commission (CQC), 2022).
Brand (2015) suggested that compliance with mandatory training ensures excellence, which is supported by Lehto et al (2017), who stated that increased staff confidence in knowledge and skills positively impacts patient care. Furthermore, the CQC expects EoLC training to be mandatory in NHS acute trusts (CQC, 2022). The first recommendation from the authors of the present study therefore is that the trust palliative and EoLC education is made mandatory for all healthcare staff, including doctors. This could also be considered regionally and nationally. Mandatory palliative and EoLC education would support the trust to deliver on national guidance, ensuring that all staff have the knowledge and skills to competently deliver high-quality care (DH, 2008; Leadership Alliance for the Care of Dying People, 2014; Healthcare Quality Improvement Partnership, 2019; National Palliative and End of Life Care Partnership, 2021). To facilitate this, a business proposal for mandatory trust palliative and EoLC education will be written and presented to trust senior leaders.
It is also recommended that attendance at future courses is promoted. This may be achieved by promoting the efficacy of the training identified in this study within the trust, care homes and domiciliary care providers. Mandating the education will also increase staff attendance.
Strengths and limitations
The sample size was small. Attendance on the courses is recommended every 3 years, which means that there are potentially 975 trust staff who can attend the courses every year. However, as the courses are currently optional, surveys could only be sent to the 238 staff who had attended the courses. This is 25% of the potential population size.
The survey response rate was poor (n=31; 13%), a limitation often seen with surveys (Alvarez et al, 2012). However, the completion rate was good with all quantitative questions answered and the only missing qualitative data were on the ‘any other comments’ from 9 respondents. Therefore, there was sufficient data from which to draw themes and conclusions. Nonetheless, future studies could increase the number of surveys sent out to further improve external validity.
The Likert scale used had 5 points, but there is evidence to suggest that a midway point tends to lead uncertain participants to this rather than make a definite choice (Chimi and Russell, 2009). However, in this study overall the midway point was not frequently used. In future studies interested respondents could also be invited to participate in a focus group to add richness to the qualitative data.
Finally, this study only addressed staff perceptions on how education improves patient care. In future studies, patient and carer perspectives on care could be explored through qualitative research such as interviews within the context of the education staff have attended. However, the emotive context of palliative and EoLC would require careful and sensitive consideration.
A strength of this study was that the qualitative findings provide meaningful data that can add to the knowledge of registered and non-registered staff and educators.
Conclusion
This service evaluation provides evidence that trust in-house palliative and EoLC education increases staff confidence levels in delivering care to patients. It also demonstrates that staff perceive that better patient care is delivered following attendance at these courses. Therefore, it is recommended that trust palliative and EoLC education becomes mandatory for all healthcare staff including doctors and that attendance at future courses is promoted.
If trust education is not made more accessible, the implications are that staff confidence levels may remain low, and there will continue to be inequitable palliative and EoLC across geographical areas. Therefore, the accessibility of good palliative and EoLC education for staff must be a priority.