

Work-related musculoskeletal disorders are highly prevalent among healthcare providers, leading to increased healthcare costs (Alnaser and Aljadi, 2019; Gorce and Jacquier-Bret, 2023; Sun et al, 2023), affecting healthcare quality and efficiency (Hartvigsen et al, 2018; Asuquo et al, 2021). Performing patient handling is associated with work-related disorders among healthcare providers due to repetitive movements, static and physical strain, and the handling of heavy loads (Fochsen et al, 2006; Knibbe and Knibbe, 2012a; Bernal et al, 2015; Amaro et al, 2018; Zenker et al, 2020). Recent research found an annual prevalence of musculoskeletal disorders (MSD) ranging from 77.2% (Sun et al, 2023) to 88.2% (Kugler et al, 2023) among nursing staff, with low back pain being the most common (Heiden et al, 2013). These disorders can lead to job dissatisfaction, burnout and health professionals leaving the field (Fochsen et al, 2006; Teixeira et al, 2022). Beyond physical inconvenience, low back pain and depression correlate with higher absenteeism rates among healthcare providers (Virkkunen et al, 2022), emphasising the need for comprehensive ergonomic practices.
To practise ergonomic patient handling as a healthcare provider, it is necessary to begin with an assessment of the patient's mobility. The patient's mobility, the extent to which the patient is able and therefore encouraged to co-operate when they need to move, is of great importance in choosing the appropriate support or method for initiating care tasks or treatment (Hignett et al, 2014). When a patient moves alone and/or can co-operate, the musculoskeletal load on the healthcare provider is expected to be significantly reduced. A thorough risk assessment during caregiver-patient interaction can enable the patient to move at their highest level of functioning. This provides patients with the opportunity to promote their rehabilitation with each interaction (Kugler et al, 2023).
Following the International Organization for Standardization guideline (ISO/TR12296) (Hignett et al, 2014) the use of a risk assessment is recommended to gain insight into the various factors that are important when moving people. The TilThermometer, widely used in northern European countries, is an example of that. It determines the care load (related to the dependence of the patient), including physical strain and the use of aids, at ward level, and provides immediate insight into the situation, with a clear report (Knibbe and Knibbe, 2012b).
The first step in using the validated TilThermometer (Buck et al, 2022) is assessing the patient's mobility, for which mobility classes are used. There are several classification systems for assessing the mobility of patients, each with its own emphasis (Kidd et al, 1995; Knibbe and Knibbe, 2012b; Harrison et al, 2013; Walters et al, 2016; Soares Menezes et al, 2017; Hoyer et al, 2018; Boynton et al, 2020; Lininger et al, 2021). Given the numerous assessments and the lack of consensus on which one to use, it is important to select the appropriate instrument for the context after assessing its feasibility for use in the workplace (Soares Menezes et al, 2017).
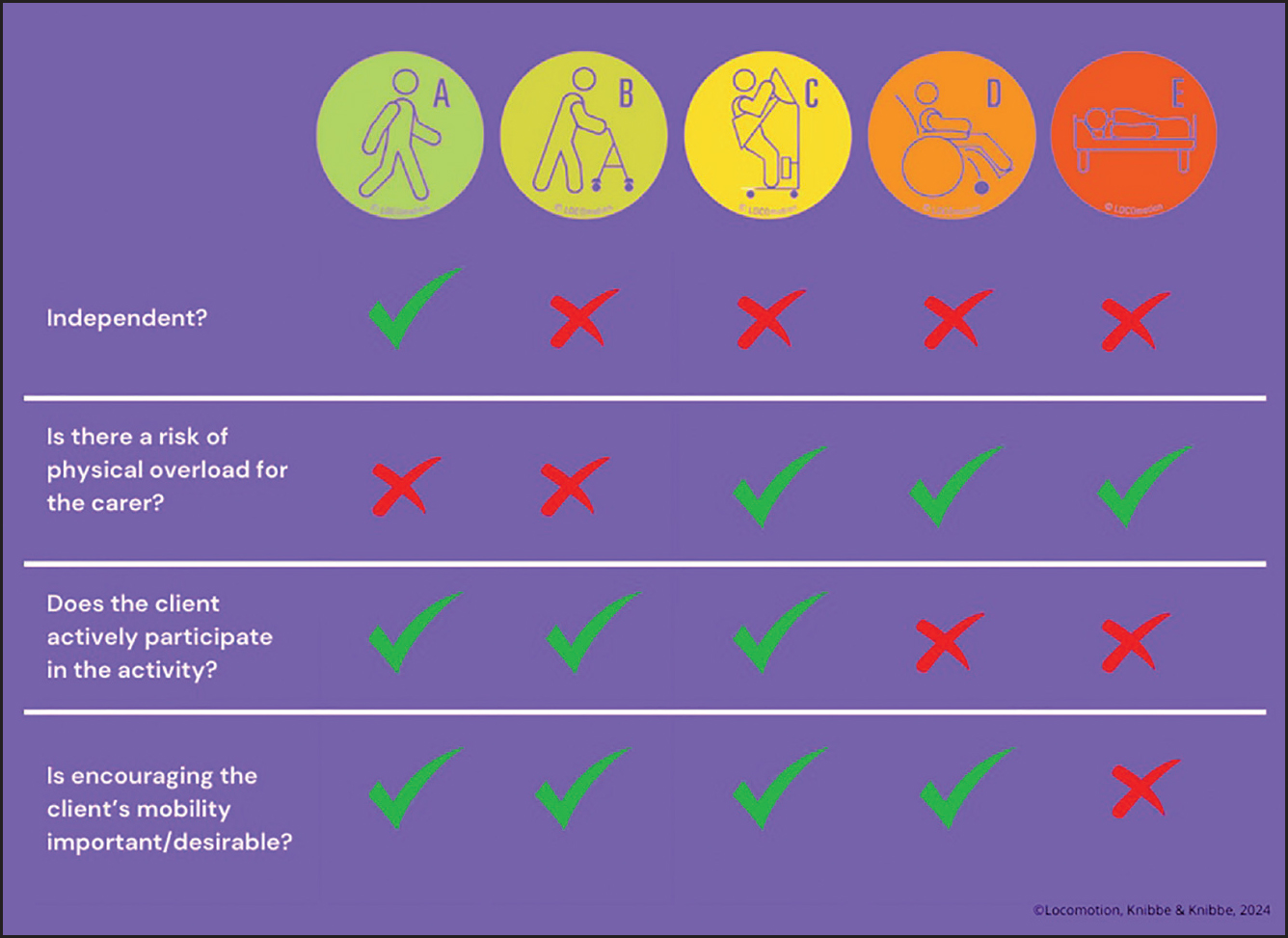
The five Mobility Classes (MK5) (see Figure 1) specifically focus on the mobility of the patient and match it with a risk profile for the occupational health of the nurse. It is described as a functional approach that primarily focuses on movement capabilities. Any underlying limitation or condition is secondary (Knibbe and Hooghiemstra, 2022). The MK5 consists of five mobility classes that are easily assigned through a concise description, accompanied by a coloured symbol (Knibbe and Hooghiemstra, 2022; Knibbe et al, 2017). The MK5 has gained trust and recognition through its extensive use in Belgium and the Netherlands and its use is considered the current best practice for categorising the mobility of patients in a user-friendly manner. This tool is also the basis for sector-specific occupational safety and health catalogues used by Dutch social partners and for inspections.Additionally, the MK5 is referenced in ISO/TR12296, a technical report that provides guidance for assessing the problems and risks associated with manual patient handling in the healthcare sector, and for identifying and applying ergonomic strategies and solutions to those problems and risks (Hignett et al, 2014). In addition, the MK5 is integrated into the international research project eUlift, a complete training module for safe patient handling (www.eulift-app.com) (Ollevier et al, 2021).
The introduction of MK5 occurred in 1993 and was deemed reliable and practical by an expert panel due to its direct linkage with the World Health Organization's (WHO) (1980) International Classification of Impairments, Disabilities and Handicaps (ICIDH), the WHO's International Classification of Functioning, Disability and Health (ICF) (WHO, 2001) and the RAI Minimal Data Set (Department ofVeterans Affairs, 2001).
The authors decided that contemporary research to support the use of the MK5 was now necessary. This study aimed to provide a substantiated view of MK5's reliability, contributing to its continued use as a professional tool in health care.
Method
This research focused on a reliability study of the MK5. To establish inter- and intra-rater reliability as sensitively as possible authentic video material was collected, enabling assessments of patient mobility by a large number of healthcare providers in a highly realistic practical setting.
Participants
A convenience sample of patients was recruited from the elderly care ward of AZ Alma Hospital in east Belgium and from the current available target population of community patients in west Flanders, Belgium. In total, 55 patients provided their informed consent to be video recorded while performing basic tasks at the request of their healthcare providers. Inclusion criteria required participants to provide informed consent. No restrictions were imposed on diagnosis, age, sex, language, mobility or cognitive functioning to ensure a broad and representative view of current patients.
Raters
A total of 200 raters (healthcare providers) were recruited to assess the mobility classes based on the video material. Both Flemish and Dutch raters participated in this study. The call for participation was disseminated through the networks of collaborating partners and via social media. Interested raters were asked to provide their contact information so that, organised in waves, specific emails with unique participation links could be sent out.
Ethical approval
Ethical approval was obtained (reference number NR EC/EH/221012-TG). A separate server room was established to store the data. The video material was made available to the raters from this secure server, via a safe connection and unique link, and was deleted after data analysis.
Procedure
Two individuals (one researcher and one affiliated with the organisation) visited 55 patients at the hospital room or at their homes to capture their mobility class on video. Patients were asked to perform a standard movement (for example, being asked to ‘go towards the toilet’) in their usual or customary manner. This moment was recorded using a camera. The recording documented how a patient's mobility class can be determined. No prior knowledge of the patients' medical histories was available. Subtitles in Dutch were added to the recordings due to occasional use of local dialects.
The video recordings served as the basis for determining the mobility class. The decision to use video recordings primarily aimed to capture a real care situation at a fixed moment in time. Regardless of the patient's health status, the recording remained unchanged, addressing a crucial concern: the stability of the patient's health condition. When conducting test-retest and inter-rater reliability assessments, the same situation was evaluated, contributing to the reliability of the chosen methodology and allowing all raters to assess the same situation, which would otherwise have been impossible. All 55 unique recordings underwent evaluation by an expert panel for content validation to determine whether a reliable assessment of the mobility class could be made based on the respective video. Although the primary aim of the MK5's authors is to evoke the conversation about mobility with the patient, based on professional knowledge, this research placed a premium on efficiently capturing authentic scenarios to encourage raters to engage in comprehensive evaluations. Despite the authors' intention to collect the same number of recordings for each mobility class, the feasibility of obtaining recordings within mobility class E (bed-bound patients) was frequently impeded by the patients' health conditions. Consequently, a deliberate selection of 40 scenarios, characterised by significant diversity, was made. The expert panel consisted of project members from eUlift, who have extensive experience with the MK5. They also determined the mobility of the care recipient based on the MK5.
The 40 final scenarios were distributed in a random sequence to the raters via the unique link, along with accompanying instructions. The raters were once again informed about the objectives and basic demographic information was collected, including country of residence, age, occupation, employment status, years of experience in health care, the classification system they normally used and experience with mobility classes. Subsequently, the raters viewed the 40 short videos independently and one by one, and assigned a mobility class by selecting the corresponding letter. An explanation of the mobility classes, indicating what each letter represented, was provided along with the videos. Additionally, the raters were asked to evaluate the difficulty of assigning the letter and were given the opportunity to leave comments. Raters were sent another link after 2 weeks to assess the 40 videos again to determine inter-rater and intra-rater reliability.
Statistical analysis
IBM SPSSv27.0 was used for data analysis. The normal distribution of raters was determined, from which descriptive statistics were derived for the previously mentioned variables. To assess reliability, inter-rater reliability and intra-rater reliability were selected, in accordance with the COSMIN guidelines for selecting the most suitable outcome measurement instrument (Mokkink et al, 2010; 2012).
The statistical analysis assessed the intraclass correlation coefficient (ICC) and the ICC framework (Shrout and Fleiss, 1979; Sim and Wright, 2005; Hallgren, 2012; Koo and Li, 2016; de Raadt et al, 2021). The ICC is a statistical metric employed to evaluate the inter-rater and intra-rater variability. It quantifies the portion of the overall variability in the ratings that can be attributed to genuine disparities between the videos, rather than random errors or variations.
Interpretation of ICC values typically follows these guidelines:
- Values below 0.5 are indicative of poor reliability
- Values falling between 0.5 and 0.75 suggest moderate reliability
- Values in the range of 0.75 to 0.90 signify good reliability
- Values exceeding 0.90 denote excellent reliability (Koo and Li, 2016).
Results
Of the 200 recruited raters, 185 signed up to take part and received the participation link. Ultimately, 147 raters completed the full assessment. Two weeks later, another unique participation link was sent to assess test-retest reliability from the same videos with 75 raters completing the full assessment. Table 1 presents an overview of the demographic data of the raters. A total of 147 responses were collected, with participants from both Belgium (58.5%) and the Netherlands (41.5%).
Table 1. Demographic data of the raters
| Characteristics | Details | Numbers and percentages (n=147) |
|---|---|---|
| Country | Belgium | n=86; 58.5% |
| The Netherlands | n=61; 41.5% | |
| Age | Mean=37.13, | |
| SD=15.26 | ||
| Minimum=18 | ||
| Maximum=66 | ||
| Professional background | Ergonomic expert | n=23; 15.6% |
| Occupational therapist | n=16; 10.9% | |
| Occupational therapist | n=16; 10.9% | |
| Physiotherapist | n=21; 14.3% | |
| Student in health care | n=47; 32% | |
| Nurse | n=13; 8.8% | |
| Healthcare assistant | n=9; 6.1% | |
| Other | n=18; 12.2% | |
| Organisational employment | Homecare | n=9; 6.1% |
| Residential care | n=25; 17% | |
| Residential care for people with disabilities | n=19; 12.9% | |
| Hospital | n=27; 18.4% | |
| Other | n=67; 45.6% | |
| Experience in health care | Years | Mean=13.72SD=13.60 |
| Classification system in use (total) | BMAT | n=2; 1.4% |
| MK5 | n=61; 41.5% | |
| Own system | n=3; 2% | |
| Other | n=10; 6.8% | |
| None | n=71; 48.3% | |
| Experience with the mobility classes | I know what it is but don't use it | n=48; 32.7% |
| I've never heard of it | n=47; 32% | |
| I use it (individually) | n=27; 18.4% | |
| It has been implemented in the workplace | =25; 17% |
Key: BMAT=Bedside Mobility Assessment Tool (Boynton, 2020)
Table 2 displays the results of the ICC to assess the reliability of using the MK5 among 147 raters across 40 distinct practical scenarios. The ICC for inter-rater reliability of the MK5 is 0.82 (95% CI, 0.99 – 0.99, P=<0.001), indicating a high level of agreement.
Table 2. Inter-rater reliability using the intraclass correlation coefficient
| Intraclass correlation | 95% CI lower bound | 95% CI upper bound | Value | Sig | |
|---|---|---|---|---|---|
| Single measures | 0.815 | 0.747 | 0.879 | 722.72 | 0.000 |
| Average measures | 0.998 | 0.998 | 0.999 | 722.72 | 0.000 |
Key: CI=confidence interval; Sig=significance
In total, 75 raters assessed the 40 scenarios twice to establish intra-rater reliability. Compared to the initial 147 raters, there was a dropout rate of 49% for re-evaluating the same video material a second time. Intra-rater reliability (Table 3) ranged from 35% (ICC=0.348; P=0.03) to 100% (ICC=1), with an average of 59% (ICC=0.59), indicating a moderate level of agreement. A maximum value of 1.0 was attributed to one unique case that displayed no variance. This scenario (T2) received identical ratings twice from all 75 raters. The results for five of the 40 scenarios – Z02; Z26;T8; Z03;T17 – (A1=assessment 1) were not found to be statistically significant and exhibited high variability, making it impossible to establish a reliable ICC. These scenarios will be subjected to an in-depth analysis through subsequent research.
Table 3. Intra-rater reliability using the intraclass correlation coefficient
| Unique patient number | ICC (average measures) | 95% CI lower bound | 95% CI upper bound | Value | df1 | df2 | P value |
|---|---|---|---|---|---|---|---|
| Z30A1 | 0.567 | 0.321 | 0.725 | 2.361 | 74 | 74 | 0.000 |
| T6A1 | 0.658 | 0.459 | 0.783 | 2.929 | 74 | 74 | 0.000 |
| Z06A1 | 0.423 | 0.084 | 0.636 | 1.726 | 74 | 74 | 0.010 |
| Z33A1 | 0.500 | 0.219 | 0.681 | 2.058 | 74 | 74 | 0.001 |
| Z02A1 | 0.290 | −0.130 | 0.553 | 1.403 | 74 | 74 | 0.074* |
| T3A1 | 0.789 | 0.667 | 0.867 | 4.725 | 74 | 74 | 0.000 |
| T19A1 | 0.678 | 0.490 | 0.796 | 3.099 | 74 | 74 | 0.000 |
| T11A1 | 0.416 | 0.072 | 0.632 | 1.704 | 74 | 74 | 0.012 |
| Z19A1 | 0.3481 | −0.031 | 0.587 | 1.534 | 74 | 74 | 0.034 |
| Z26A1 | 0.228 | −0.228 | 0.514 | 1.292 | 74 | 74 | 0.136* |
| Z34A1 | 0.504 | 0.225 | 0.684 | 2.098 | 74 | 74 | 0.001 |
| T12A1 | 0.636 | 0.422 | 0.770 | 2.896 | 74 | 74 | 0.000 |
| Z18A1 | 0.406 | 0.067 | 0.622 | 1.695 | 74 | 74 | 0.012 |
| Z14A1 | 0.675 | 0.485 | 0.795 | 3.051 | 74 | 74 | 0.000 |
| T21A1 | 0.615 | 0.394 | 0.756 | 2.689 | 74 | 74 | 0.000 |
| T8A1 | 0.312 | −0.094 | 0.567 | 1.448 | 74 | 74 | 0.057* |
| Z22A1 | 0.708 | 0.537 | 0.815 | 3.397 | 74 | 74 | 0.000 |
| Z03A1 | 0.129 | −0.275 | 0.419 | 1.176 | 74 | 74 | 0.244* |
| T15A1 | 0.400 | 0.053 | 0.620 | 1.670 | 74 | 74 | 0.014 |
| T5A1 | 0.56 | 0.301 | 0.723 | 2.256 | 74 | 74 | 0 |
| Z28A1 | 0.498 | 0.203 | 0.683 | 1.980 | 74 | 74 | 0.002 |
| T16A1 | 0.663 | 0.468 | 0.787 | 2.974 | 74 | 74 | 0.000 |
| Z15A1 | 0.584 | 0.345 | 0.736 | 2.425 | 74 | 74 | 0.000 |
| T17A1 | −0.069 | −0.704 | 0.327 | 0.936 | 74 | 74 | 0.612* |
| Z25A1 | 0.474 | 0.178 | 0.665 | 1.941 | 74 | 74 | 0.002 |
| T4A1 | 0.701 | 0.528 | 0.811 | 3.357 | 74 | 74 | 0.000 |
| Z16A1 | 0.572 | 0.322 | 0.729 | 2.329 | 74 | 74 | 0.000 |
| T13A1 | 0.773 | 0.641 | 0.856 | 4.495 | 74 | 74 | 0.000 |
| Z27A1 | 0.406 | 0.067 | 0.623 | 1.694 | 74 | 74 | 0.012 |
| T14A1 | 0.720 | 0.556 | 0.823 | 3.691 | 74 | 74 | 0.000 |
| T18A1 | 0.661 | 0.465 | 0.785 | 2.973 | 74 | 74 | 0.000 |
| Z04A1 | 0.362 | 0.008 | 0.592 | 1.595 | 74 | 74 | 0.023 |
| Z12A1 | 0.567 | 0.318 | 0.726 | 2.323 | 74 | 74 | 0.000 |
| T20A1 | 0.574 | 0.329 | 0.730 | 2.364 | 74 | 74 | 0.000 |
| Z31A1 | 0.674 | 0.484 | 0.794 | 3.187 | 74 | 74 | 0.000 |
| T7A1 | 0.522 | 0.250 | 0.696 | 2.129 | 74 | 74 | 0.001 |
| Z17A1 | 0.724 | 0.565 | 0.825 | 3.651 | 74 | 74 | 0.000 |
| T10A1 | 0.642 | 0.431 | 0.774 | 2.767 | 74 | 74 | 0.000 |
| T1A1 | 0.692 | 0.514 | 0.806 | 3.368 | 74 | 74 | 0.000 |
| T2A1 | 1.0002 | 0.000 |
Key: CI=confidence interval; df=degrees of freedom; ICC=intraclass correlation coefficient *=not significant; 1=lowest ICC; 2=highest ICC
Additional exploratory statistical analysis did not reveal significant differences in the assessments based on factors such as hospital scenarios versus home-care scenarios, the age of the raters, the country of residence, or whether they had experience with a classification system.
Discussion
The primary objective of this study was to assess the inter-rater and intra-rater reliability of using the MK5 in healthcare settings, because it plays a crucial role in evaluating the mobility of patients and determining appropriate care methods.
The sample included 147 raters, with representation from both Belgium (58.5%) and the Netherlands (41.5%), reflecting diverse profiles, healthcare experience and familiarity with classification systems. This diversity underscores the MK5's applicability in different healthcare contexts within these countries.
To assess mobility classes accurately within a large group of raters and ensure internal accuracy, the authors designed this study to depict a realistic and common healthcare situation. The use of test-retest and inter-rater reliability assessments, where the same scenario was evaluated by different raters at different times, contributed to the method's reliability. To mitigate potential fluctuations in a patient's health condition and minimise bias among raters, video recordings were employed. Furthermore, no medical record knowledge was provided, allowing all raters to view the recordings with the same level of patient history information. Therefore, we recognise that stronger reliability is likely achieved with experienced healthcare providers possessing greater patient history knowledge.
The primary focus of the research was the inter-rater reliability of the MK5 across 40 practical scenarios. A high level of agreement among raters was observed. This indicates a strong consensus among raters when using the MK5. The narrow confidence interval range reinforces the precision of this estimate. These findings affirm that the MK5 can consistently assess patient mobility across diverse healthcare scenarios. In addition to inter-rater reliability, intra-rater reliability with 75 raters re-evaluating the same scenarios was assessed. Despite a 49% dropout rate for re-evaluation, a moderate level of agreement, with an average ICC of 0.59, was noted. Some scenarios exhibited perfect agreement, while a small number showed lower reliability due to high variability or nonsignificant results. These scenarios warrant further investigation in future research.
Acknowledging study limitations, the 49% dropout rate for intra-rater reliability assessment may have influenced the results. Future research should aim to minimise this dropout rate to enhance the robustness of the findings. Additionally, although the study included participants from Belgium and the Netherlands, its generalisability to other healthcare systems or regions requires more exploration. Furthermore, despite the intention to collect approximately the same number of recordings for each mobility class, more challenging situations in the healthcare context were encountered. Since mobility class E guarantees comfort as a top priority and patient activation is no longer a priority, these are the patients with the most severe pathologies, and they were also the most challenging to approach because of physical and/or verbal and/or cognitive impairment. For this reason, only one video was included where a clear class E patient was visible. However, it was noted that mobility class E was assigned to other videos as well. A possible explanation of why class E was still assigned may be because it was visually apparent that there were five classes, which could have led to socially desirable responses and the occasional assignment of an E.
The high inter-rater reliability of the MK5 implies its value as a tool for health professionals to consistently assess patient mobility. This is particularly crucial in healthcare settings where patient-handling decisions rely on mobility assessments. Reliable assessments can enhance patient care, reduce healthcare provider injury risk, and improve overall care quality (Hignett et al, 2014; Karppi et al, 2022).
Because the MK5 is considered best practice in Belgium and the Netherlands, the authors advocate for broader adoption of assessment tools in healthcare institutions to improve patient care and mitigate healthcare provider health issues. This research underscores the importance of practical ergonomic training in this context (Sousa et al, 2023).
The accurate assessment of patient mobility is a pivotal component of health care, aiming to optimise patient capabilities and minimise physical strain on healthcare providers. This MK5 reliability study, using video recordings, reinforces its effectiveness in assigning mobility classes consistently. This research aligns with previous literature advocating for the use of assessments (Soares Menezes et al, 2017; Karppi et al, 2022) and their integration into healthcare organisations.
As demonstrated in the study by Chen et al (2023), the global health and economic burden of low back pain in the working-age population is significant, but it is also imperative to underscore the repetitive and substantial physical strain endured by healthcare providers in the course of their the job (Fochsen et al, 2006; Knibbe and Knibbe, 2012a; Bernal et al, 2015; Amaro et al, 2018; Zenker et al, 2020). In order to prevent these work-related musculoskeletal complaints among healthcare providers, the authors emphasise the added value of assessment tools that promote ergonomic training and provide necessary assistive devices (Koppelaar et al, 2013; Andersen et al, 2019; Miller et al, 2022).
Conclusion
This study provides evidence of the high reliability of MK5 in evaluating patient mobility in healthcare settings. The tool can be used consistently by different healthcare providers, regardless of their experience, contributing to better patient care and safety. The MK5 serves as an informative tool for initiating conversations about mobility for both healthcare providers and patients. It should be administered contextually and with care, not as a final objective, but as a means to enhance healthcare outcomes.
KEY POINTS
- Patient handling is connected to the high degree of work-related musculoskeletal disorders
- The assessment of the patient's mobility is recommended by ISO/TR12296
- An assessment of the patient's mobility is the first step in safe patient handling
- The use of reliable assessments in health care is crucial
- The MK5 Mobility Classes is a reliable tool for assessing patient mobility in healthcare settings
CPD reflective questions
- How do you assess your patients' mobility in your area of work?
- What are the key challenges involved in assessing patients' mobility?
- What are the implications for patients and healthcare providers when assessing patients' mobility?
- Do you use a valid tool to assess your patients' mobility? How could use of the tool be improved?