

Vascular access devices (VADs) are used universally within health care, and caring for these devices remains an important part of the role of all health professionals (Welyczko, 2020). Peripheral venous cannulas (PVC) are the most commonly used intravascular device and for many reasons are considered integral to patient care (Mermel, 2017; Drugeon et al, 2023). However, they continue to pose a significant and an arguably under-recognised infection risk (Blauw et al, 2019; Buetti et al, 2022; Drugeon et al, 2023).
Royal Devon University Healthcare NHS Foundation Trust (formerly Royal Devon and Exeter NHS Foundation Trust, which started the audit project) has been undertaking continuous VAD bacteraemia surveillance for more than 20 years. To ensure a consistent approach to identifying VAD bacteraemias, audit and surveillance practitioners apply the strict criteria outlined in the Protocol for Surveillance of Hospital-Acquired Bacteraemia (Nosocomial Infection National Surveillance Service (NINSS), 2001) (see Box 1). These criteria allow the Trust to review trends in the incidence of VAD bacteraemias over the 20 years' worth of data held. Only cases in which the primary source of the bacteraemia is deemed to be an intravascular device, with no other apparent extravascular sources, and that meets these criteria, are included in the data.
Definitions of bacteraemia
| Bacteraemia (including fungaemia) must meet one of the following criteria | |
|---|---|
| Criterion 1 | One or more recognised pathogens that are not common skin flora* isolated from one or more blood cultures |
| Criterion 2 | At least one of the following clinical signs or symptoms** of infection within 24 hours of a positive blood culture being taken: fever (skin temperature ≥38°C), chills, rigors, or hypotension (systolic blood pressure ≤90 mmHg) and an organism that is common skin flora isolated from: |
Source: Nosocomial Infection National Surveillance Service, 2001
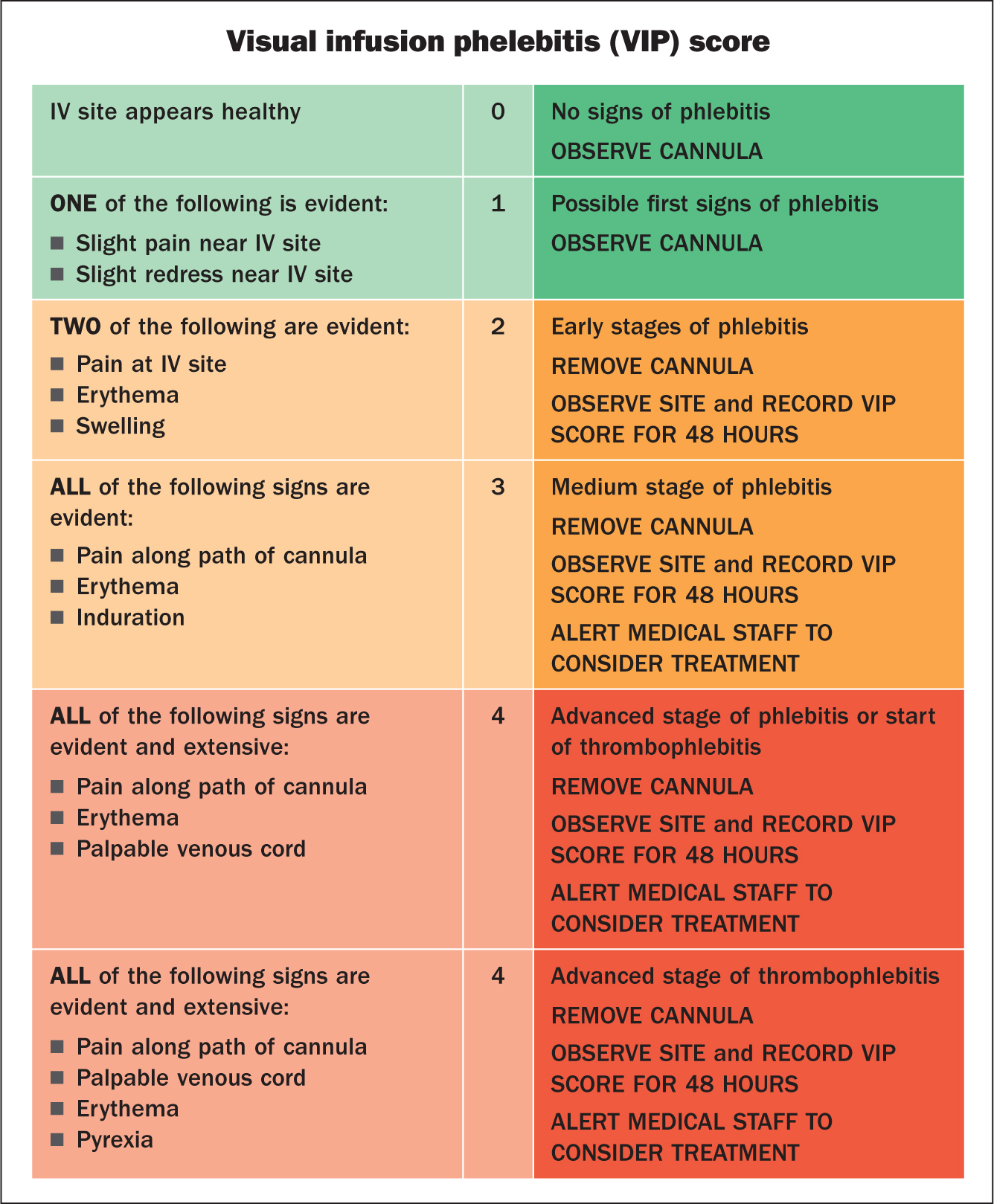
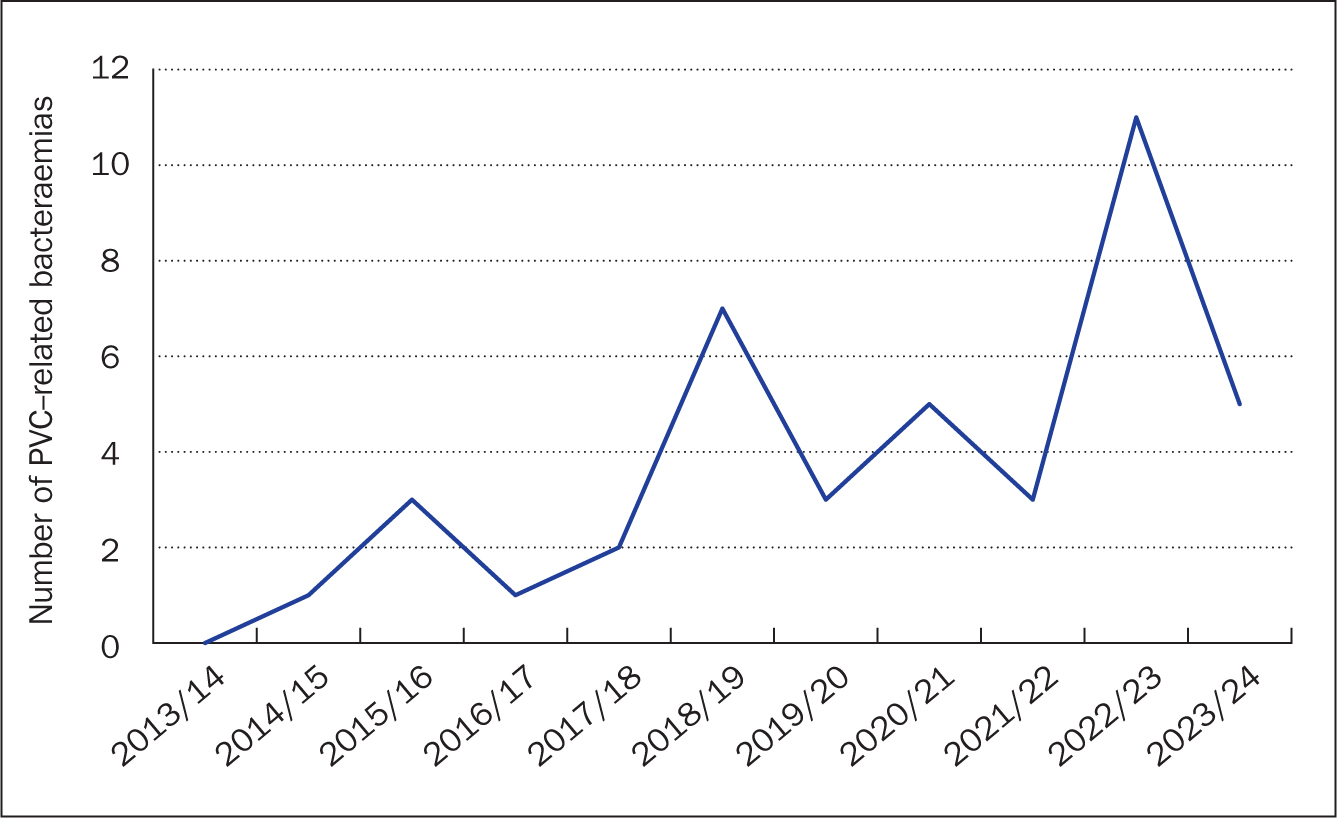
Despite previous collaborative improvement initiatives implemented across the Trust, there has been an overall increase in the incidence of PVC bacteraemias since 2013/14. Data for the financial year 2022/23 showed a steep rise between 2021/22 and 2022/23 – an increase of 267%, which is the highest incidence since 2004/05. Thorough analysis of these cases identified a series of recurrent learning themes, particularly a lack of compliance in the recording of at least daily visual infusion phlebitis (VIP) scores (Figure 1) and prolonged PVC dwell times. The trust's VAD policy recognises a maximum recommended dwell time of 96 hours (Webster et al, 2019). However, the policy allows for extended dwell times, providing that there are no signs and symptoms of infection, that the site is regularly monitored with at least daily VIP scores recorded, and that a rationale for extending dwell time is clearly documented. In many cases, a lack of daily VIP scores being recorded led to the first concerns being escalated when a pustule or severe phlebitis was apparent. Compliance with the recording of VIP scores and documenting the rationale for longer dwell times as per Trust policy may have prevented some of these cases.
Staphylococcus aureus is part of the normal human skin flora residing on the skin and mucous membranes of most healthy individuals (UK Health Security Agency, 2020). The insertion of any VAD poses a potential infection risk, offering a pathway for opportunistic microorganisms, particularly those that are part of the normal skin flora, to enter the bloodstream via broken skin (Clare and Rowley, 2021; Munoz-Mozas, 2023; Osório et al, 2023). These risks highlight the vital importance of adequate skin preparation and maintenance of all VADs in the prevention of infection.
S. aureus is generally considered to be the single most prevailing causative microorganism for PVC-related bacteraemia (Austin et al, 2016; Blauw et al, 2019). In England, it has been mandatory to report S. aureus bacteraemia since 2001; in 2005, mandatory enhanced surveillance of meticillin-resistant S. aureus (MRSA) bacteraemia was implemented and, in 2011, this was extended to include meticillin-sensitive S. aureus (MSSA) bacteraemia (UK Health Security Agency, 2020).
Since the financial year 2018/19, S. aureus has been identified as the causative organism in all cases of PVC bacteraemias within the Trust, with MSSA being the single prevailing causative microorganism. An MSSA bacteraemia alone carries a significant healthcare burden for both the individual and the healthcare service (Bhatt et al, 2021). In 2022/23, the UK case fatality rate for an MSSA bacteraemia was 21.9%, with a mortality rate of 5.1 deaths per 100 000 population (UK Health Security Agency, 2024). MSSA bacteraemias are also associated with prolonged lengths of hospital stays, with associated financial and operational implications for trusts (Trinh et al, 2011; Blauw et al, 2019; Allen and Direito, 2025).
Initiating any form of change within health care is often complex and challenging. When implemented effectively with engagement from multidisciplinary teams, quality improvement projects play a vital role in improving care and enhancing patient safety while optimising clinical processes, directly leading to a reduction in hospitals infection rates (Jones et al, 2019; Endalamaw et al, 2024).
Consequent to the identified rise in rates of MSSA bacteraemias across England, which exceeded pre-pandemic levels (UK Health Security Agency, 2024), coupled with an increasing incidence of PVC bacteraemias across the Trust, the Infection Prevention and Control (IPC) Team deemed it critical to implement a quality improvement project aimed at improving compliance with Trust policy and reducing PVC bacteraemias.
Methods
The initiative involved a multimodal approach that included a survey, poster campaign and education sessions. However, before embarking on the design and implementation of the programme, the Trust's IPC Team wanted to clarify whether there had been any changes to the relevant equipment or products used during the insertion, maintenance or removal phases of caring for PVCs since the steep rise from 2021/22. No changes in equipment or products were identified since 2021/22 that may have explained the steep increase in PVC bacteraemia cases observed across the Trust.
The IPC Team then retrospectively reviewed all cases of PVC-related bacteraemias over the preceding 3 years to identify areas the project should focus on (Table 1). Despite previous research studies identifying links between bacteraemias relating to PVCs inserted in the emergency department or by the ambulance service (Trinh et al, 2011; Blauw et al, 2019; Drugeon et al, 2023), there was no association evident from the Trust's data. The vast majority of PVC bacteraemias occurred in those inserted in the inpatient setting, so this was the area chosen to focus on.
| 2021/22 | 2022/23 | 2023/24 | |
|---|---|---|---|
| Incidence | |||
| Total number of PVC-related bacteraemia | 3 | 11 | 5 |
| Resistance | |||
| Meticillin-resistant Staphylococcus aureus (MRSA) | 1 | 0 | 0 |
| Meticillin-sensitive Staphylococcus aureus (MSSA) | 2 | 11 | 5 |
| Categorisation of infection | |||
| Hospital onset healthcare associated (HOHA) | 2 | 10 | 5 |
| Community onset healthcare associated (COHA) | 1 | 1 | 0 |
| Community onset community associated (COCA) | 0 | 0 | 0 |
| Age | |||
| <65 years | 1 | 3 | 3 |
| ≥65 years | 2 | 8 | 2 |
| Sex | |||
| Male | 2 | 6 | 4 |
| Female | 1 | 5 | 1 |
| Anatomical placement of causative PVC | |||
| Hand | 1 | 3 | 0 |
| Forearm | 1 | 2 | 2 |
| Antecubital fossa | 1 | 5 | 3 |
| Foot | 0 | 1 | 0 |
| PVC duration | |||
| <96 hours | 0 | 5 | 1 |
| ≥96 hours | 2 | 4 | 4 |
| Unknown | 1 | 2 | 0 |
| Clinical setting of PVC insertion | |||
| Emergency department or ambulance service | 2 | 3 | 1 |
| Inpatient area | 1 | 7 | 4 |
| Unknown | 0 | 1 | 0 |
PVC=peripheral venous cannula
A local point prevalence survey across the Trust conducted in 2022 found suboptimal compliance with both daily VIP score recording and the documentation requirements to record the rationale for PVCs with dwell times of more than 96 hours. Compliance scores on both of these aspects were calculated to provide a baseline compliance prior to implementing the initiative. The survey included a total of 781 patients who between them had 436 PVCs; of these, 378 PVCs had been in situ for less than 96 hours and 58 PVCs for more than 96 hours.
Having recognised the ongoing staffing pressures across the Trust's acute hospitals, and the difficulty in releasing staff for training, it was decided to adopt a ward-based approach. In April 2022, following the initial local point prevalence survey, the Trust merged with a neighbouring Trust; the latter did not routinely undertake VAD bacteraemia surveillance and had different policies mandating practice. Therefore, a decision was made to implement the quality improvement initiative only across the merged Trust's largest acute hospital site where continuous VAD bacteraemia surveillance had been undertaken for many years. This would allow the true impact of the project on the incidence of PVC bacteraemia to be evaluated.
A multimodal PVC improvement initiative was developed and implemented by the IPC Team with support from the Vascular Access Team. The initiative included an educational poster highlighting the serious infection risk associated with PVCs, while detailing key prevention messages from the Trust's VAD policy. Posters were to be displayed in all clean utility rooms (where intravenous medications are stored and/or prepared) across all inpatient areas, the intention being that they would act as an aide-mémoire to support the reduction of PVC bacteraemia.
A face-to-face teaching session, complementing the poster, was also delivered by the IPC Team to promote best practice, with a specific focus on areas of recurrent learning and prevention of PVC bacteraemias. The teaching sessions were designed to be concise and memorable, and included references to individualised clinical area compliance scores as identified in the 2022 survey. Recent case studies from the Trust's largest acute hospital site were also included, along with clinical photographs of the infected PVC sites to make the sessions more stimulating. Multiple sessions were offered to each clinical area, with good uptake, to encourage and enable the inclusion of the majority of staff. Those who attended the sessions were then encouraged to disseminate their learning to peers to raise awareness and discussion of the topic.
The teaching resources used for each ward were also disseminated to clinical nurse managers and clinical matrons, together with a request for their support in the improvement drive. It was hoped that the involvement of multidisciplinary teams and collaborative working would ensure a sustained reduction in PVC bacteraemias.
The initiative was aimed at both registered and unregistered health professionals who have direct involvement in patient care. Implementation of the initiative commenced in June 2023.
Results
Both written and verbal feedback following the teaching sessions was obtained from each clinical area. The feedback was positive, and many staff members were astounded that the case studies presented had occurred in their hospital. The sessions had the desired impact and helped initiate discussions within the clinical areas regarding PVCs and the severity of the risks associated with their use. The individualised compliance scores for each clinical area also gained the interest of the clinical nurse managers and their teams, providing the motivation they needed for improvement across their areas.
A further local point prevalence survey was conducted across the acute hospital site in November 2023 to evaluate the impact of the initiative on compliance: this involved recording at least daily VIP scores and complying with the documentation requirements for PVCs with a dwell time of more than 96 hours. The survey included 797 patients and 479 PVCs; 434 PVCs less than 96 hours and 45 PVCs more than 96 hours.
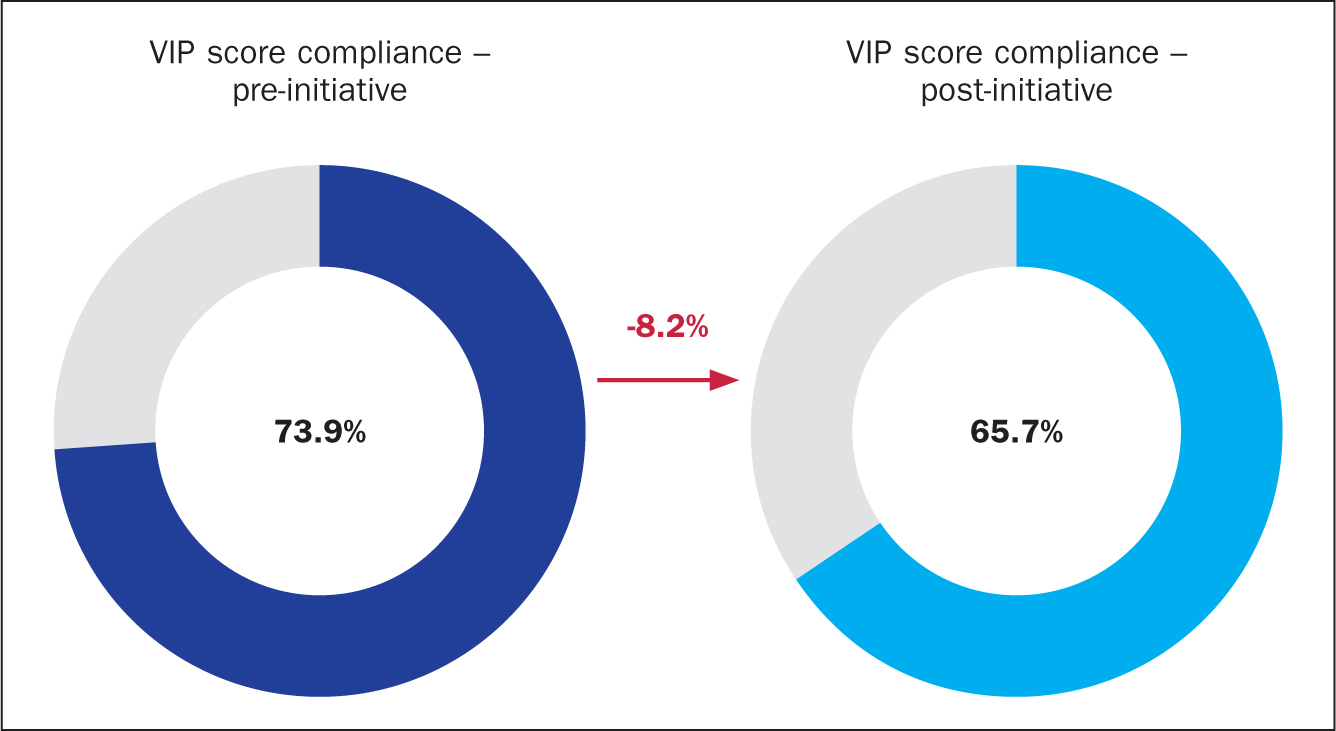
The results showed a compliance score of 65.7%, with the recording of at least daily VIP scores post-initiative, reflecting an unfortunate decrease in compliance compared with the pre-initiative score of 73.9% (Figure 2); the Trust's target was 100%. Despite this, some clinical areas achieved a significant improvement in compliance, with one ward attaining an increase of 53.3% in its score.
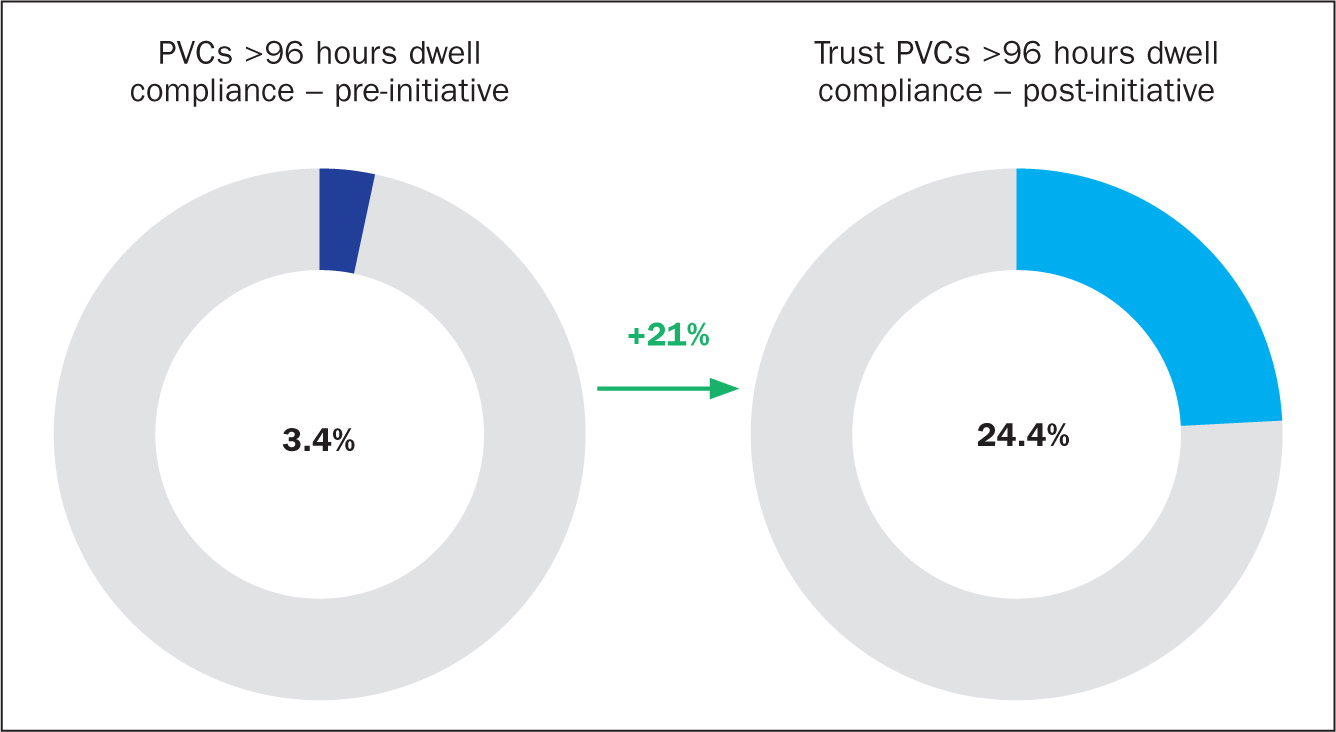
With regard to the documentation requirements for PVCs with more than 96 hours' dwell time post-initiative, the compliance score was found to be 24.4% (Figure 3); the Trust's target was 100%. This reflected a significant improvement of 21% compared with the pre-initiative compliance of 3.4%, with some clinical areas seeing a 100% improvement in their score.
Despite the results post-initiative reflecting a decrease in compliance in recording at least daily VIP scores, the VAD bacteraemia surveillance data for October-December 2023 was encouraging. The data highlighted a reduction of 50% in the incidence of PVC bacteraemia when compared with the previous quarter, reflecting the lowest recorded incidence of PVC bacteraemia since January-March 2022. This was a hopeful sign and suggested that the quality improvement drive may have had the desired effect.
Discussion
Following on from noting a reduction in compliance with at least daily VIP scores post-initiative, further promotion and wider support of this PVC improvement drive was essential if the IPC Team were to obtain what it had initially set out to achieve. The PVC improvement drive and the outcomes were subsequently presented at the Trust's Infection Prevention and Decontamination Assurance Group (IPDAG), with the result that the improvement initiative gained the attention and support of the Trust's senior colleagues and its governance and safety teams. The presentation to IPDAG resulted in a number of actions, including a request for all divisions to support the improvement drive and develop their own action plans on how to improve compliance, and to present these at the following IPDAG meeting.
Additional education resources in a variety of formats were developed by the IPC Team to raise further awareness of the impact that PVC bacteraemias and their associated complications have on both patients and the Trust as a whole. This included the creation of a Trust-wide educational screensaver promoting PVC care and required documentation, as well as an educational piece for inclusion within the Trust's weekly staff update and the Trust-wide monthly iBulletin newsletter. It was hoped that using a range of educational resources containing the same content and images, would assist in reinforcing positive behaviours and improve compliance with Trust policy. In addition, to gain much-needed senior support to drive forward the PVC improvement initiative, the project and the results were presented at the trust-wide ‘Care Matters’ monthly meeting attended by the Trust's band 7 staff and above. This use of multiple resources and modes of delivery also helped to ensure that a wider selection of healthcare staff across different bands were targeted.
The Royal Marsden Manual (Lister et al, 2020) recommends that PVCs are replaced when clinically indicated instead of routinely at 96 hours, unless manufacturer recommendations specify otherwise. The Trust policy reflected this with a 96-hour recommended maximum dwell time, but permitted extended dwell times providing that there were no signs and symptoms of infection, that at least daily VIP scores were recorded and that a rationale for choosing to extend the dwell time was documented. Due to an evident relationship noted within the Trust data between bacteraemias and PVCs with longer than 96 hours' dwell time, alongside poor compliance with regular monitoring of PVCs highlighted from the latest survey results, a review of Trust policy was undertaken. It was decided to revert to instigating a maximum dwell time of 96 hours with routine replacement of PVCs. Although the IPC Team recognises that the Trust will be among the minority of those reverting to previous guidelines, it was felt this was the right thing to do, given the current situation regarding PVC bacteraemias in the Trust. Additionally, Trust policy did not stipulate routine dressing changes for PVCs with dwell times of longer than 96 hours; some PVCs were known to have been left in situ for 16 days (384 hours) with no documented dressing changes made within that time frame.
National Institute for Health and Care Excellence (NICE) (2014) guidelines specify that all vascular access device dressings should be changed a minimum of every 7 days. A lack of weekly dressing changes and routine skin decontamination could lead to an increased load of microorganisms, particularly skin flora, at the insertion site; this increases the risk of microorganisms entering the bloodstream via broken skin leading to bacteraemia (Hicks et al, 2023). Prolonged use of PVCs and a lack of routine dressing changes, particularly in cases of excessive dwell times, may have had an associated infection risk and account for some of the PVC bacteraemias the Trust has seen.
It was hoped that reverting policy to a blanket maximum dwell time of 96 hours would highlight the issue and place the focus on the basics of PVC care, helping to improve compliance, with at least daily VIP scores recorded, and would reduce the incidence of PVC bacteraemia.
As per the recognised VIP scoring system, any PVC with a VIP score of 2 or more has to be removed and re-sited if required. No guidelines exist within the VIP scoring system to monitor a site for early signs of phlebitis or residual burden of microorganisms; if undetected and not addressed, these can lead to infection at the site following removal of the device. This lack of monitoring following removal of a PVC, in cases when a VIP score of 2 or more was recorded, led to the first concerns being escalated when a pustule or severe phlebitis was apparent, at which point the patient was already bacteraemic.
As per the Royal Marsden Manual (Lister et al, 2020), early detection and prompt removal of a PVC device is crucial in preventing PVC-related bacteraemias. Therefore, a new requirement to continue to record VIP scores for sites for 48 hours' post-removal of a PVC in cases where a VIP score of 2 or more is recorded was instigated, as reflected in Figure 1. It is hoped this will help with earlier identification and escalation of clinical concerns of infection and help to prevent localised infection deteriorating into a bacteraemia.
As a result of the IPC Team's ongoing persistence with the PVC improvement drive, along with wider collaborative support from both the clinical and governance teams, the Trust is now starting to see the desired reduction in incidence of PVC bacteraemias (Figure 4). Data have shown a 54.5% decrease in the incidence of PVC bacteraemias in 2023/24 compared with the previous year. Moreover, the IPC Team reported zero PVC bacteraemias for the January-March 2024 quarter, the lowest recorded incidence over 2 years. Although the IPC Team did not initially achieve the desired results from the improvement project alone, the initiative has shown how collaborative working can greatly benefit and enable successful change across health care. The Trust hopes to sustain the current reduction in the incidence of PVC bacteraemias in future.
Conclusion
Identifying areas for improvement and implementing quality improvement projects are key to improving the safety, effectiveness and experience of patients within the UK healthcare systems. As these results show, collaborative working is essential for securing the success of quality improvement projects, it is also vital to have a clear approach, and to use clear and effective communication, to change accepted attitudes and practices surrounding the use and management of VADs.
Although the IPC Team had to implement a return to previous guidelines to improve the monitoring of PVCs and help raise awareness of the potential severity of complications associated with the use of PVCs, this could be clinically justified. Taking a step back and placing more focus on the ‘back to basics’ of VAD care was crucial and, alongside the improvement drive, it has led to a reduction in the incidence of PVC bacteraemias. The initiative has also helped to prevent ‘just in case’ PVCs from being inserted, empowering health professionals to insert PVCs only when clinically indicated and encouraging the removal of ‘idle’ PVCs that are no longer required.
Only time and continuous PVC bacteraemia surveillance will tell if the changes have had a long-term impact in sustaining a reduction in PVC bacteraemias. Awareness of, and education about, VADs, and an understanding of correct selection, competent insertion and dwell time duration remain key in preventing VAD-associated bacteraemias.
When undertaking the research for this project, there appeared to be a lack of research into the true incidence of PVC bacteraemias. PVC bacteraemias remain incredibly costly to treat, with huge implications on both a patient's mental and physical health. The financial resources spent treating cases of PVC bacteraemia could be better utilised conducting more comprehensive research studies into the prevention of future cases.
Further research studies could assist in informing the creation of standardised educational training materials, and standardised policies for best practice across the NHS. PVC-related bacteraemias and the severity of some cases remain an under-acknowledged and under-recognised topic within health care.