

In 2021, the Australian Commission on Safety and Quality in Health Care released a national Clinical Care Standard to promote safe use of peripheral intravenous catheters (PIVCs).1 This was in response to overwhelming evidence that PIVC outcomes globally are unacceptable.2 As Australian health care providers are expected to implement and comply with the standard, quality improvement efforts are underway in many settings to improve PIVC care and outcomes.
In Brazil, the National Health Surveillance Agency (ANVISA) is responsible for promoting activities relevant to the protection of the population's health. In 2017, ANVISA published Measures for Prevention of Healthcare-Associated Infections; this guide presents evidence-based measures, adjusted to the reality of Brazilian health care, that must be taken to mitigate health care–associated infections in health care facilities. It includes recommendations to prevent bloodstream infections caused by PIVCs.3
A historic perception of PIVCs as low risk has led to suboptimal care.4 Evidence over the past decade confirms PIVCs pose a bloodstream infection risk like central venous catheters when volume of usage is considered.5,6 Therefore, PIVC assessment and decision making must be evidence based to reduce risks and improve patient care.7,8
Implementation of evidence-based care bundles increases adherence to interventions and improves patient outcomes, such as reduced catheter dwell time and complication rates.8,9,10 Professional knowledge and experience, convenience, and the patient's clinical progression all impact PIVC decisions.11 Exploring quality improvement studies reporting positive outcomes could increase awareness among health care professionals, improve adherence to evidence-based practices, and enhance the quality of PIVC care.
Background
PIVCs are the most common invasive device in health care; 70% of patients require at least one during their hospital stay.12 Repeated insertion attempts are common, and over one-third of PIVCs fail before treatment completion, due to phlebitis, infiltration, occlusion, or dislodgement.5 High failure rates could be reduced with a systematic approach for post-insertion management.5
The Infusion Nurses Society recommends regular PIVC assessment to prevent catheter-related infections—examining the catheter site for skin and dressing integrity, daily review of clinical necessity, and prompt removal when appropriate.13 Daily discussions with the health care team and patient and/or family regarding PIVC need are essential. Evaluation should include documentation of insertion, daily assessment, and removal to ensure consistency, quality, and safety of care.13,14 Despite recommendations of standards and guidelines, hospitals often develop local PIVC policies contrary to research evidence. Additionally, nurses may not always be aware of or adhere to best practice.4,15
The I-DECIDED® tool brings evidence-based assessment and management to the point of care with a simple mnemonic.16 The tool has robust content validity and high inter-rater reliability for PIVC assessment as well as good feasibility and acceptability.17 It has been validated and implemented in the adult context in Australia,9,17 cross-culturally adapted for use in Brazil,18 and implemented in the pediatric context in Brazil. Across adult and pediatric settings, its implementation has yielded positive outcomes, particularly in the reduction of unused catheters and PIVC complications.9
The tool is non-prescriptive; rather, it scaffolds assessment-informed decision making and empowers nurses to act on their decisions. Staff are prompted to check each item of the tool but maintain flexibility for their actions. For instance, staff are asked to consider removal if the PIVC has not been used in the past 24 hours or has no plans for use in the next 24 hours. The tool does not specify dwell time because staff often leave in a well-functioning and asymptomatic PIVC, regardless of policy, if a patient is difficult to cannulate or if treatment will soon be completed.19
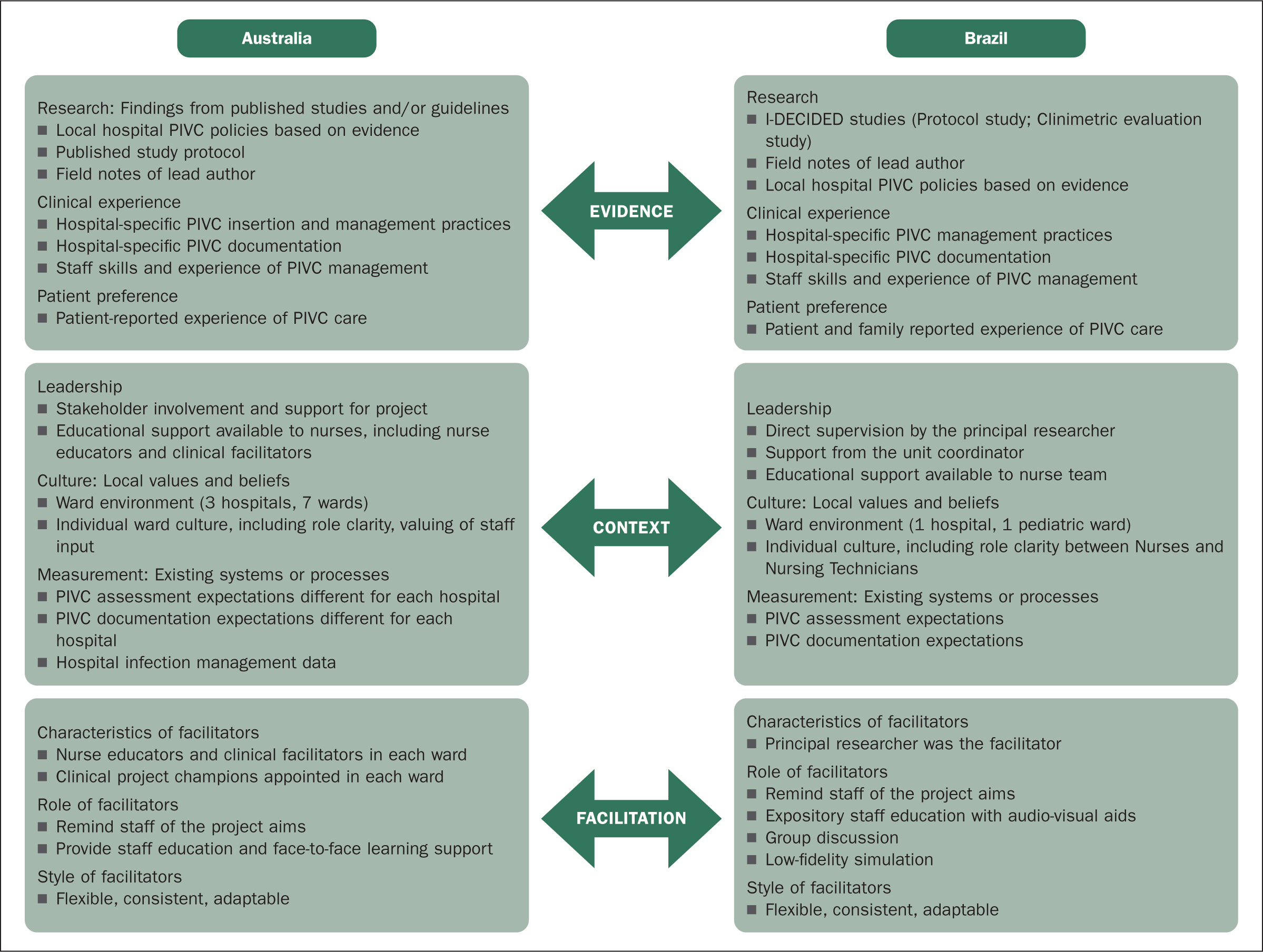
Implementation frameworks and models can enhance nurses' understanding of quality improvement processes and resultant patient outcomes.20 In this paper, we evaluate the implementation of the I-DECIDED® tool using the Promoting Action on Research Implementation in Health Services (PARIHS) framework.21 We discuss processes for successful implementation (evidence, context, facilitation) and propose future directions.
The Australian study received Human Research Ethics Committee (HREC) approval from Queensland Health (HREC/17/QPCH/47), Griffith University (Ref No. 017/152), and St. Vincent's Health and Aged Care (Ref No. 17/28). The Brazilian study was approved by the HREC of the Universidade Federal of Santa Catarina (Ethical Approval No. 5.965.146; Ethical Review Presentation Certificate: 64135122.9.0000.0121). All patients provided informed consent for their data inclusion. The Standards for Quality Improvement Reporting Excellence version 2.0 (SQUIRE 2.0) guidelines22 guided reporting of the outcomes.
Australia
In Australia, the tool has been trialed among adults with PIVCs in 3 hospitals, resulting in fewer idle catheters and insertion site complications and improved documentation.9 The PARIHS framework was used prospectively to plan the implementation (see Figure 1).21
First, the investigator (a postdoctoral researcher) invited the chief nurse and infection control lead from several hospitals to invite nurse unit managers to participate in the study. The original plan was to trial the tool in 3 adult public hospitals; however, 1 hospital withdrew prior to commencement due to the concurrent implementation of an electronic patient record; therefore, a private hospital volunteered as the third site. The sample size of 7 wards (3 medical, 3 surgical, and 1 infectious diseases) ensured sufficient PIVCs were available for assessment.
Each hospital was in a different health service, so trial documents needed modification to meet local governance and hospital documentation requirements. The investigator was a registered nurse employed by the university rather than the health services, so a credentialling process for scope of practice for non-employees was completed before the study began.
Next, the investigator reviewed each hospital's PIVC policies and met with key stakeholders to plan the implementation to fit within the context of each participating ward. Pretrial PIVC documentation varied greatly between hospitals, so the decision to implement a trial paper form incorporating the tool met with mixed responses. Nurse unit managers, educators, infection control staff, clinical facilitators, and ward champions were all invited to contribute to development of the trial form to encourage buy-in; this was well received. Throughout the study, the investigator met bimonthly with stakeholders and visited each ward regularly to maintain momentum and answer questions.
An interrupted time-series study was conducted over 11 months, with data collection in Phases 1 and 3 and the education and implementation roll-out in Phase 2. A research assistant collected PIVC data every 2 weeks using REDCap,23 with inter-rater reliability checks repeatedly undertaken among the investigator, research assistants, and ward nurses.17 In Phase 1, nurses assessed PIVCs as per local policy. In Phases 2 and 3, nurses followed the I-DECIDED® tool on the trial form to assess the PIVC each 8-hour shift and decide to continue, troubleshoot, or remove the PIVC, based on their assessment.
During Phase 2, the investigator conducted multiple short education sessions during afternoon shift handover. These enabled staff to ask questions about the tool and the trial form. Throughout the study, nurse educators, nurse unit managers, and local champions provided ongoing education and support. Laminated posters of the tool were placed in all patient bedside folders. Completed sample trial forms were displayed in staff rooms, and badge cards were provided to all staff. Some ward champions created additional posters to promote the project in their own ward. For example, the infectious diseases ward promoted the tool as an innovative way to reduce PIVC-related bloodstream infections.
Nurses reported that the tool increased their awareness of the need to remove unnecessary PIVCs; this was reflected in the reduced prevalence of idle PIVCs. However, many nurses expressed frustration with the extra paperwork, and compliance with the form was low in some wards. Despite this, PIVC documentation improved by 49% overall. Following the study, 1 hospital modified their PIVC assessment form to include the tool, another hospital continued to use the tool for PIVC education, and the other hospital reverted to the previous assessment (phlebitis tool only).
Brazil
Following cross-cultural adaptation into Brazilian Portuguese, 18 the tool was implemented in a pediatric unit of a teaching hospital in southern Brazil. The nursing staff consisted of 7 registered nurses (university training), 18 nursing technicians (technical nurse training), and 4 nursing assistants (secondary school). The unit uses an electronic patient record system; registered nurses document each patient's care every 24 hours, while nursing technicians or assistants document care per shift.
A quasi-experimental, interrupted time-series study assessed the impact of the tool on PIVC assessment, care, decision making, and documentation. Data collection spanned 7 months, 3 pre-intervention and 3 post-intervention time points.
During the intervention period, education was conducted to introduce the tool to the nursing team: firstly, the researcher (PhD student) delivered a theoretical presentation, explaining the tool's purpose and applicability through interactive discussions aided by audiovisual resources, followed by group discussions. Next, a low-fidelity simulation was conducted using a mannequin with a PIVC inserted, along with a clinical case containing the access characteristics, simulating a hospitalized child. In total, 3 different clinical cases were developed and randomly distributed to professionals. The researcher demonstrated how to use the tool in clinical practice and how to document the PIVC assessment and decision-making process. Professionals were instructed to read the clinical case, then proceed to the mannequin to assess the PIVC, perform necessary care, make a decision about appropriate actions, and document this in a fictitious medical record.
Both stages had an average duration of 40 minutes and took place during all 3 shifts in a reserved environment when patient care demands were lower. Two education sessions were conducted per team to ensure participation of the maximum number of professionals and avoid disruptions in patient care. All nursing team members participated in the training.
The researcher provided badge cards to all staff for quick reference during patient assessments. Posters showcasing the tool were placed in documentation areas within the unit to serve as reminders for proper documentation (see Figure 2). Although planned for 2 months, the educational intervention concluded in 1 month due to the collaborative efforts of the team and the single unit involved. The researcher remained available to address any questions or concerns.
Initially, some staff expressed concerns about potential added workload and time constraints. However, with simulation, they realized that implementing the tool would not overly burden their daily routines. Unfortunately, integrating the assessment form into the existing electronic system was not feasible. As a result, professionals had to document PIVC assessments and decisions alongside other patient records, which made the documentation process somewhat laborious.
A key factor facilitating implementation was the low-fidelity simulation, effectively demonstrating to the professionals that adopting the tool would not hinder patient care. Another positive factor was the distribution of badge cards; there was a high adoption rate, and it was observed that professionals consulted the cards during patient care. The use of electronic record helped prevent potential data loss.
Discussion
Clinical assessment is a foundation of nursing practice, and a systematic, evidence-based approach to assessment and decision making enables care to be standardized and replicable across clinical settings and patient groups. As PIVCs are ubiquitous in clinical practice, they are often treated with benign neglect, but high rates of catheter failure have enormous personal and economic consequences for patients and health care organizations that could be mitigated with improved assessment and decision making by nurses. The importance of regular and systematic assessment is unquestionable, particularly with the growing trend toward clinically indicated PIVC replacement, supported by international vascular access guidelines.13, 24, 25 However, assessment alone is insufficient without targeted decision making. The I-DECIDED® tool prompts device decisions based on the assessment: continue, troubleshoot, change dressing, or remove PIVC. Using I-DECIDED®, clinicians routinely reassess the PIVC indication and function, change substandard dressings, and remove it when no longer required or at the first sign of complications.
Implementation of the tool in the 2 contexts demonstrated that early detection or prevention of undesirable PIVC complications is achievable with standardized assessment. Both studies witnessed a reduction in idle PIVCs, decreased complications, improved dressing quality, and a significant improvement in documentation following implementation. Furthermore, implementation in different contexts (adult units in Australia, a pediatric unit in Brazil) confirms that the tool is useful and relevant in diverse health care settings.
Despite the importance of evidence-based management for improving patient outcomes, implementation is frequently complex and challenging, particularly when professionals lack awareness of risks associated with PIVCs.14 Implementing and maintaining change requires time, effort, and resources, with one of the main challenges being obtaining consensus among a variety of disciplines and amid competing hospital priorities.26 In the Australian study, the PARIHS framework was used to plan the implementation, and in the Brazilian study, the framework was used to retrospectively evaluate the implementation, as per Hill et al.27 Next, we describe how the PARIHS framework can provide strategies for the implementation of the tool in practice.
Evidence
The I-DECIDED® tool was developed from a synthesis of evidence, clinical guidelines, phlebitis tools, decision tools, and PIVC bundles, and the original study protocol was published prior to study commencement.16 In addition to robust content validity and high inter-rater reliability, the tool demonstrated good feasibility for use in daily practice and acceptability among professionals; the average time to complete assessments was 2 minutes.17
In the Australian study, a review of hospital policies and procedures for PIVC assessment and documentation established the baseline expectation for nurses. This was followed by repeated stakeholder meetings to ensure the implementation plan would be congruent with the care delivery model in each ward. In Brazil, retrospective analysis identified the importance of the existing electronic patient record system and staff experience levels for driving PIVC management.
Context
Despite the diverse contexts, implementation of the tool led to a significant reduction in complications and prevalence of idle catheters in both studies. Idle catheters are a waste of staff time and resources, while PIVC complications increase inpatient length of stay and treatment costs.28 Implementation of the tool demonstrated a reduction in adverse consequences; further studies are needed to determine the potential cost savings. A French study that analyzed the cost effectiveness of a PIVC maintenance bundle versus standard approach in preventing unscheduled removal due to complications showed that the bundle was the most effective and economical strategy, with an average saving of €42 per patient.29
Previous researchers have revealed that patients and caregivers are often not included in PIVC decisions,30 with a corresponding higher incidence of idle catheters.31 Authors of both the Australian and Brazilian studies found that patients' knowledge of their PIVC improved following implementation of the I-DECIDED® tool. Authors of further studies could identify whether increased patient knowledge can reduce PIVC complications and improve patient outcomes.
Facilitation
Health professionals are motivated to ensure patient safety and avoid harm, but incorporating multiple changes into clinical practice can lead to change fatigue.32 To improve the integration of evidence into practice, it is necessary to support professionals' knowledge of and adherence to evidence-based guidelines and practice change. Local facilitators and project champions are essential for project success, given that professionals who perceive the benefits of change tend to view this process positively.33
Both implementation studies were led by early career nurse researchers (1 postdoctoral student, 1 PhD student), so identification of local key stakeholders who could help plan and drive the implementation was imperative. Regular connection with nursing managers, nurse educators, and local champions is needed to drive engagement in any practice change. In an implementation project, different levels of engagement from the targeted end users can be anticipated, and preemptive strategies for minimizing resistance should be built into the rollout.34 For example, the provision of education and ongoing support for the change over several months can reduce the perception of burden by some stakeholders.34 In the Australian study, resistance to change from some nurses was countered by setting clear expectations for PIVC assessment, including an emphasis on the timely removal of idle catheters as a smart strategy to reduce bloodstream infections. In the Brazilian study, nurses expressed concern that the assessment would be time consuming, but the simulation exercises reassured them that the I-DECIDED® assessment took no more time than usual practice.
Limitations
Our evaluation of the implementation of the tool has certain limitations. Without supportive line managers and enthusiastic nurse champions, quality improvement projects often fail once the drivers for change are removed; we have not measured longer-term sustainability. While implementation in our countries showed positive findings, other countries may have different experiences, particularly in cultures where nursing autonomy and decision making is not widely valued.
Implications for practice
We encourage other researchers to use an implementation framework to guide clinical quality initiatives.35 The positive findings from implementation of the I-DECIDED® tool support its adoption. With the reduction in complications and idle catheters, the tool shows promise for reducing catheter-related infections and improving patient outcomes. The tool encourages nurses to advocate for patient safety by informing and empowering patients to be involved in decisions about their PIVCs.36
Receiving harm-free care is a patient right and an institutional responsibility, especially where harm is avoidable. The authors encourage clinicians to consider implementing the tool to improve quality of care, with future research to deepen understanding of the implementation benefits, such as potential cost reduction for hospitals. The tool's wording makes it suitable for assessment and decision making of other invasive devices (eg central venous catheters, urinary catheters), but this has not been tested. Translations into languages other than English and Brazilian Portuguese have been completed but not tested.
Conclusion
Providing evidence-based, point-of-care guidance for assessment and decision making, the I-DECIDED® tool enables standardized PIVC practice across clinical settings and patient groups. Implementation of the tool demonstrated positive results in Australian and Brazilian contexts by reducing idle catheters and complications and improving documentation. Further adoption could ensure high-quality device care across health care settings.