

Basic life support (BLS) is crucial in the event of a cardiac arrest (European Resuscitation Council, 2021; Resuscitation Council UK (RCUK), 2021) and BLS training is of international concern (Dick-Smith et al, 2021). In hospitals, nurses are often the first responders to a cardiac arrest, providing BLS, which is a mandatory skill. Nursing students are involved directly in caring for acutely ill patients (Smith and Rushton, 2018), who are at risk of cardiac arrest, and require training to ensure that they can assist and deliver BLS if required.
The self-confidence of the learners in performing a practical skill is important (Aoyama et al, 2013). Swift et al (2022) acknowledged that the development of self-confidence is not related to just one learning episode, but that self-confidence is the outcome of scaffolded learning that relates to theory and practice. Nurse educators need to find strategies to instil confidence to enable the students to deliver BLS under pressure (Smith and Hamilton, 2015).
It is well known that providing effective BLS increases survival rates (Sangavi et al, 2015). Currently, BLS training is updated annually using a low-fidelity simulation (LFS) resuscitation manikin and follows behaviouristic learning theory, where learning occurs through observation, imitation and modelling (Bandura, 1977). BLS training allows students to learn through observation and deliberate practice. This type of training also follows experimental theories such as Kolb's theory, which involves learning from experience (McLeod, 2023). This theory allows participants to re-enact scenarios to enhance learning and gain experience in that area of interest.
Nurse educators use various methods of simulation to enable learners to practise their BLS skills. The Nursing and Midwifery Council (NMC), as part of the standards for pre-registration education and training, identified simulation as a method of education, using a variety of modalities (NMC, 2023). This allows the opportunity for repetition, feedback and evaluation, developing safe and effective practice in a safe learning environment. Simulation also promotes the development of confidence (Cioffi et al, 2005; Rushton, 2015), to provide care in emergency situations.
BLS training traditionally uses LFS, consisting of static tools with no interactions (Jeffries, 2012). Truszewski et al (2016) emphasised the increased use of medium-fidelity simulation (MFS) for BLS training by providing the user with more feedback about their performance. High-fidelity simulation (HFS) is also used in BLS and involves computerised manikins that provide realistic physiological responses (Bruce et al, 2009; Toubasi et al, 2015), adding increased reality (RCUK, 2015). Simulation also provides the opportunity to develop essential skills such as team working and communication skills (Gordon and Buckley, 2009; Handeland et al, 2021).
HFS follows a constructivist approach, allowing the participants to actively engage in realistic scenarios and gain instant feedback. LFS has limited capability to provide realism for nursing students, because they do not have the experience to be able to create a mental picture in simulated scenarios. However, Kim et al (2016) stressed that all levels of simulation help to build student confidence, with LFS building knowledge, MFS building competence and HFS building performance.
The usefulness of enhanced levels of simulation in building confidence has been widely reported (Oermann et al, 2010; Rahmawati and Sulistiya Ningsih, 2020; Mather and McCarthy, 2021). It is worth remembering that HFS has its own limitations, because it can be costly to co-ordinate, and restrictive in terms of time and location (Yu et al, 2021). Nevertheless, virtual reality technology (VR) can potentially be an alternative because it requires fewer resources and is very portable, compared with other forms of simulation (Kardong-Edgren et al, 2019). VR technology is becoming more prominent in education but at the moment is not routinely used in BLS teaching. Table 1 summarises the different types of simulation, along with some advantages and disadvantages.
Table 1. Simulation types
| Level | Characteristics | Examples | Disadvantages |
|---|---|---|---|
| Low fidelity (LFS) | Used to acquire basic psychomotor skills in a simple procedure or physical examination that only simulates one part of the body (Alconero-Cameraro et al, 2021) | Basic manikin for cardiopulmonary resuscitation (CPR), cardiac auscultation, or limb for catheterisation | Lack of realism in scenarios |
| Medium fidelity (MFS) | Offers more realism, which enables the instructor to manage basic physiological variables, with the aim of developing competency (Alconero-Cameraro et al, 2021) | Manikin connected to a less complex pre-established software with the aim of achieving the development of competency, eg Sim CPR feedback manikin | |
| High fidelity (HFS) | Integrates multiple physiological variables for the creation of realistic clinical scenarios with life-size manikins (Alconero-Cameraro et al, 2021) | Sim ManMeti man | Costly equipment and lack of portability (Yu et al, 2021) |
| Virtual reality (VR) | A computer-generated, three-dimensional virtual environment, which is immersive if using goggles or headset, or non-immersive if there are screens around the learner to project information (Hamad and Jia, 2022)Uses fewer resources and more portable than other methods (Kardong–Edgren et al, 2019) | VR Lifesaver app (Resuscitation Council UK) | Can be high cost affecting accessibilitySome users complain of headache and eye strain (Hamad and Jia, 2022) |
The RCUK (2024) has the VR Lifesaver app, which enables the learner to become immersed in the cardiac arrest scenario. In Italy, VR technology has been trialed to enhance BLS training (Almousa et al, 2019), alleviating the deterioration of skills, while other studies have shown how VR can enhance confidence (Rushton et al, 2020). The use of this type of technology also tackles the well-known issues with restrictions of time, place, and personnel associated with conventional courses (Almousa et al, 2019).
With the NHS technological revolution, it is increasingly important that we prepare our learners for the future workforce of the NHS. The digital revolution and rapid development of technology in recent decades have greatly influenced the shape of education, providing tools for creative learning (Guze, 2015).
Some literature suggests that using higher levels of immersion produces better results for learning, improving knowledge and skills, and achieving higher confidence levels (Rushton et al, 2020). It is important to ensure that learners are prepared for the workplace and that they have adequate knowledge, skills, competence and confidence to carry out clinical skills. However, some nurses still lack confidence in emergency scenarios, which is a global issue. Previous international studies in Europe and America have identified the deficit in confidence relating to BLS (Onan et al, 2018; Mather and McCarthy, 2021). Yet, the links with the level of simulation and the confidence associated with BLS remain debated. Literature suggests that an increase in the ability to apply practical skills equates to an increase in confidence (Arnold et al, 2008; Bruce et al, 2009).
Confidence in performing BLS skills is fundamental. According to Bandura's (1989) theory, the learner's self-efficacy can enhance or impede their performance. Nursing students often lack knowledge and confidence (self-efficacy) in relation to critical-care nursing and are often apprehensive about practice placements in these areas (Rushton, 2015). Cardiac arrests can occur in a variety of settings, but it is the emergency acute situation that often leaves the students feeling fearful, or unprepared.
Aim
The study objective was to examine whether the environment (clinical skills lab, classroom, HFS suite) or the level of simulation (LFS or HFS) in BLS training affects the students' confidence.
Methods
This quasi-experimental cohort research project was conducted in the School of Health and Society. Ethical considerations were adhered to, and institutional ethical approval was granted by the university research and ethics committee. Quantitative data were collected using a prevalidated confidence tool. A quantitative approach was most appropriate for analysing trends in confidence levels (Coghlan, 2014). The study compared the environments currently used to teach BLS within the institution: clinical skills lab using LFS manikins, standard classroom using LFS manikins, and HFS suite using high-fidelity manikins. Equator research reporting guidelines were adhered to (https://www.equator-network.org/reporting-guidelines/strobe) and extensions for simulation-based research included (Cheng et al, 2016).
Sample
The study sample was gathered using purposive sampling, a deliberate non-randomised method, sampling a specific group of people (Watson, 2015). There were 125 participants, 123 female and 2 male participants recruited from a cohort of second-year student nurses, adult field of practice, who had completed the first year of the programme and had attended three clinical placements. All participants had received BLS training in their first year and were due for an annual update.
The study was designed with behavioural theories in mind, as deliberate practice and practising of BLS skills would support performance improvement. Constructivist theories ensured that participants were encouraged to reflect on their BLS learning to support their skills in decision-making in the BLS scenarios. It was also important to think about the development of confidence and, from a social cognitive perspective, learners were encouraged to practise BLS skills in a variety of simulated environments.
All participants had been in the simulation areas prior to the study and were familiar with the surroundings. The orientation to all simulation facilities takes place in year 1 of the programme and the different facilities are used at various times throughout the timetabled simulated practice sessions. However, the previous BLS training session was carried out in a clinical skills room.
Design of the project
The BLS training was divided into three different areas to be able to compare the confidence in the three areas, and participants were allocated in their pre-set tutor groups to a specific area. The BLS session content was the same, regardless of the environment (Table 2).
Table 2. Basic life support simulation sessions
| Session plan |
|---|
|
The areas consisted of a clinical skills lab (n=40 students), standard classroom (n=52 students) and an HFS suite (n=33 students). The hypothesis was that the clinical skills lab and the high-fidelity suite would show higher levels of confidence, because these were environments with which the students were most familiar.
The students were informed about the purpose and requirements of the project during a lecture, and written participant information sheets were also provided with further details of the study. The participant information sheet gave details on the nature, purpose and methods of the study. Students were assured of confidentiality and anonymity.
Informed consent was obtained before inclusion in the study and the participants were made aware of their right to withdraw at any time (Coghlan and Brannick, 2014). Each student was allocated a unique identification number, which was stored on a password-protected computer. Any student who did not wish to participate would still receive the mandatory update but was not required to complete the questionnaire.
Questionnaire
The questionnaire, which gathered data regarding the confidence of the students, was adapted with permission from the pre-validated confidence tool designed by Arnold et al (2009). The validity and reliability of this was tested during a pilot study. The pilot study had 15 participants and tested the design of the questionnaire, allowing for any necessary amendments. The post-training questionnaires had a 5-point Likert scale ranging from ‘no confidence’ to ‘confident’ with items assessing confidence levels in BLS, so participants could self-evaluate their levels in relation to performing the BLS algorithm. The data obtained were then coded (Table 3).
Table 3. Questionnaire items and data coding
| Questionnaire items | Coding |
|---|---|
|
1.0 No confidence2.0 Little confidence3.0 Some confidence4.0 Very confident5.0 Totally confident |
Data analysis
Quantitative data from the questionnaires were analysed using the statistical software package SPSSv23, and descriptive statistics were extracted to illustrate the mean scores for each of the variables. The data were then analysed using R (www.r-project.org/about.html), which provided a variety of statistical and graphical techniques. A Kruskal-Wallis Test was selected because the data were non-parametric.
Findings
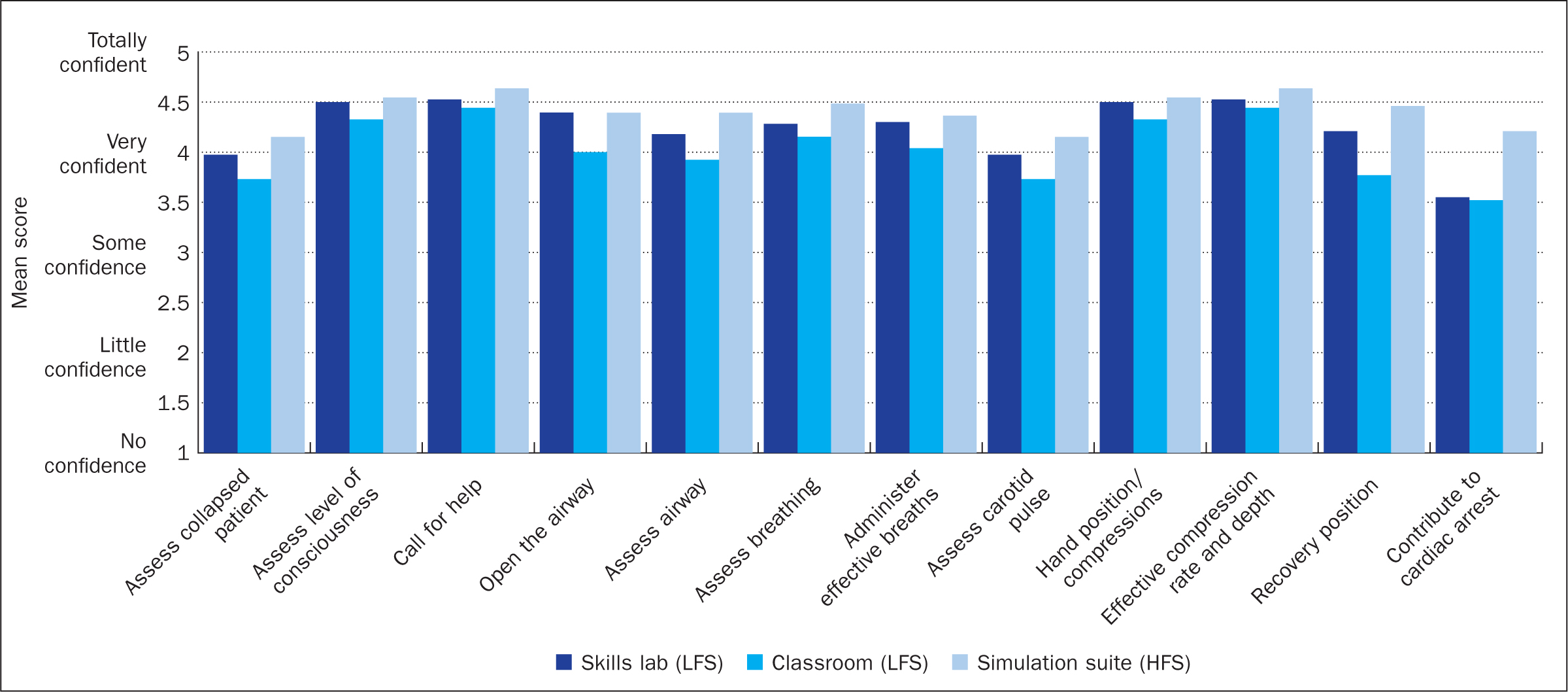
The results show that the HFS suite had a significant impact on confidence levels (Table 4 and Figure 1). All items showed that the simulation suite (HFS) was the most effective in terms of developing confidence levels. This area gained all the highest mean scores (4.1515 to 4.6364), apart from opening the airway (head tilt chin lift). The environment within which participants mostly had mid mean confidence scores (3.5500 to 4.5250) was the skills lab (LFS). Interestingly, opening the airway scored the highest mean value in this environment (4.3947). The lowest mean scores were achieved by participants who performed BLS in the classroom environment (3.5192 to 4.4423). Statistical significance was seen in assessing a collapsed patient, performing opening the airway (head tilt, chin lift), assessing airway, checking pulse, recovery position and contribution in a cardiac arrest, all resulting in P<0.05 (Table 4).
Table 4. Mean scores for each of the variables
| Mean confidence scores | Skills lab (LFS) | Classroom (LFS) | Simulation suite (HFS) | P value (significance <0.05) |
|---|---|---|---|---|
| Assess collapsed patient | 3.975 | 3.7308 | 4.1515 | 0.0268 |
| Assess level of consciousness | 4.5 | 4.3269 | 4.5455 | 0.296 |
| Call for help | 4.525 | 4.4423 | 4.6364 | 0.593 |
| Open the airway | 4.3947 | 4 | 4.3939 | 0.0185 |
| Assess airway | 4.1795 | 3.9231 | 4.3939 | 0.0268 |
| Assess breathing | 4.2821 | 4.1538 | 4.4848 | 0.133 |
| Administer effective breaths | 4.3 | 4.0392 | 4.3636 | 0.102 |
| Assess carotid pulse | 3.975 | 3.7308 | 4.1515 | 0.00518 |
| Hand position/compressions | 4.5 | 4.3269 | 4.5455 | 0.199 |
| Effective compression rate and depth | 4.525 | 4.4423 | 4.6364 | 0.366 |
| Recovery position | 4.21 | 3.77 | 4.46 | 0.000246 |
| Contribute to cardiac arrest | 3.55 | 3.52 | 4.21 | 0.000246 |
HFS=high-fidelity simulation environment; LFS=low-fidelity simulation environment
The study's design meant that pre- and post-statistics were not compared, as its purpose was to examine the effect of the different environments. The findings clearly show HFS to be more significant in confidence levels; however, it is not possible to identify whether there was an increase in confidence following the session because these were not recorded pre-training. Further research will examine pre- and post-confidence levels data so that correlations can be made regarding the impact that different environments have on individual students.
Discussion
The study's aim was to explore the accustomed levels of simulation used to teach BLS, and to determine the effect of the simulation environment on students' confidence in performing BLS.
The findings from the study have revealed some key issues related to students' confidence in BLS skills. A significant finding has been the impact of an HFS environment on learners' confidence levels. Developing confidence in BLS training is paramount to the health professional's ability to provide quality care in a stressful situation. The NMC Standards of Proficiency for Registered Nurses (NMC, 2018), item 4.13, identifies the need to demonstrate knowledge, skills, and confidence to provide BLS. The fact that HFS has a bigger impact on confidence levels proves its usefulness as a pedagogical approach, and in the development of the confidence to be able to carry out the skills required in the event of a cardiac arrest. It is well known that HFS helps to develop confidence and enhances the reality of the training scenario. This significantly contributes to the development of confidence in psychomotor critical thinking and leadership skills (Jeffries, 2012; Yuan et al, 2012).
An unexpected finding in the study was the fact that, in the skills room, participants scored opening the airway (head tilt chin lift) as highest – this may be due to witnessing this previously in the skills room, during demonstrations, and because they felt more confident in applying this skill within the skills room. Supporting this, international research carried out by Al Gharibi and Arulappan (2020) identified the importance of developing hands-on skills associated with BLS. They concluded that HFS is not always superior to LFS because it depends on the task required and the learner's initial level. Ultimately, an increased ability to perform the kinesthetic, practical skills required for BLS equates to an increase in confidence (Bruce et al, 2009).
Of note is that, in the HFS setting, there was a significant increase in participants' confidence in being able to contribute to a cardiac arrest situation within a hospital setting. The reality of the HFS setting allows learners to be prepared for real-life situations, in a clinical practice environment. This also allows them to develop critical thinking and transferable knowledge for clinical practice (Handeland et al, 2021), as well as increasing their confidence and competence (Al Gharabi and Arulappan, 2020). Conversely, Yu et al (2021) reported that some studies found that HFS could cause students to have blind confidence, overestimating their abilities, with clinical diagnosis errors linked to overconfidence. In support of this, Massoth et al (2019) also considered that HFS is not superior to LFS and leads to overconfidence. Nevertheless, studies such as that of Mutlu et al (2019) are supportive of the value of HFS in improving students' clinical skills.
Overall, the hypothesis that the clinical skills lab and the high-fidelity suite would show higher levels of confidence is supported by the data. Confidence is built by gathering key skills required in the clinical area, which include teamwork, communication, interprofessional and clinical decision-making skills (Preston and Flynn, 2010). This then provides the learners with the knowledge and skills to be more confident in dealing with an emergency, such as a cardiac arrest. HFS has been seen as a key educational tool for developing these crucial skills for some time (Gordon and Buckley, 2009). However, with ever-evolving advances in technology, it is necessary to consider other possibilities for enhancing the students' experience and confidence in BLS by using new pedagogical approaches.
This includes considering alternative approaches to teaching and learning – and currently HFS is widely recognised as a beneficial tool for learning. The NMC supports up to 600 simulation hours (NMC, 2023). It is thought that using a variety of advanced simulation technologies, including more recent additions such as augmented reality (AR) and virtual reality (VR), can further immerse the learners in their learning experience and build confidence (Rushton et al, 2020). Nevertheless, it is important to acknowledge the limitations of VR technologies, such as the lack of face-to-face communication with patients or other members of the team (Baniasadi et al, 2020). Non-technical skills, such as communication, are essential when caring for a patient who has suffered a cardiac arrest (Calder et al, 2017).
Educationists need to embrace innovative technologies, to ensure that learners are getting the best possible experience and that they build their knowledge and confidence to be able to carry out BLS. Using different technologies or simulated scenarios may better prepare them for delivering BLS in a real-life situation (Preston and Flynn, 2010; Yuan et al, 2012), as health professionals need to feel confident in BLS in their workplace.
Driving forces, such as patient safety and limited clinical placement areas, have also increased the need to incorporate technology-driven simulation in nurse education programmes (Higham and Baxendale, 2017). Integration of new technologies such as VR and simulation has been viewed as crucial in bridging the theory–practice gap. Simulation and VR technology have gained significant attention within the healthcare and medical education industries around the world in recent years (McGhee et al, 2011).
Limitations
Pre- and post-statistics were not analysed, as the purpose of the study was to examine the effect of the environment on participants' confidence. Therefore, it is not possible to determine whether there was an increase for individual participants following the session.
Conclusion
The findings of this study support the value of HFS and have revealed that BLS in the HFS simulation suite had a greater impact on learners' confidence levels. All the variables showed that the simulation suite (HFS) was the most effective in terms of increasing students' confidence levels. Of note is that the variable opening the airway scored the highest mean value for confidence levels in the low-fidelity clinical skills lab environment. Overall, the lowest mean scores were achieved by participants who performed BLS in the classroom environment, suggesting that the setting in which BLS training is delivered is an important element in ensuring that confidence is developed. Statistical significance was observed in several of the variables, which showed the impact of training on the nursing students' confidence levels. The researchers identified that further exploration of a variety of technologies and settings may be required to enhance the fidelity/realism in the learning environment and to instil more confidence, making the learner better prepared for the provision of BLS in a real-life cardiac arrest.
KEY POINTS
- Basic life support (BLS) is a mandatory skill for all nurses and health professionals
- Regular training and BLS practice are essential to improve confidence
- Healthcare education needs to embrace a variety of technologies and settings to enhance the realism in the learning environment and instil more confidence, to ensure that learners are better prepared for the provision of BLS in the event of a real-life cardiac arrest
- High-fidelity simulation is a key educational tool for developing crucial BLS skills
- Effective use of new technologies, such as virtual reality and simulation has been seen as crucial in bridging the gap between theory and practice
CPD reflective questions
- How is basic life support (BLS) education delivered in your pre-registration programme?
- How can this learning enhance your practice and confidence to support the care you deliver to people affected by a cardiac arrest?
- What are the challenges of integrating enhanced levels of simulation into your BLS learning?