

Vital signs assessment is an important nursing function that allows early identification of the deteriorating patient (Kamio et al, 2018). The regular monitoring of vital signs can alert the nurse to any developing clinical events, thus allowing timely detection of deterioration and improved patient outcomes (Brown et al, 2014; Richard et al, 2018). Up to 80% of patients exhibit a deterioration in vital signs in the 24 hours prior to an adverse event (Trocki and Craig-Rodriguez, 2020). The presence of three or more critically abnormal vital signs has been associated with a higher mortality risk (Bleyer et al, 2011).
Vital signs assessment and escalation of care is fundamental to patient safety and the first step in patient rescue (Bucknall et al, 2017). However, research has found that only half of patients who meet the criteria for emergency medical review are actually reviewed because nurses do not call for assistance (Bucknall et al, 2013; Bingham et al, 2015). In an Australian study, patients who fulfilled emergency medical review criteria at the time of vital sign assessment were more likely to die in hospital or within 30 days (Bucknall et al, 2013).
Despite the importance of vital signs assessment, numerous studies have found this task is often neglected. For example, in a retrospective analysis of 49 unexpected intensive care admissions from a general hospital ward in The Netherlands, the most frequent root cause of the clinical deterioration was failure in patient monitoring (van Galen et al, 2016). Other studies have reported similar findings such as: 72% of patients having a difference between their actual respiratory rate and that which was documented (Semler et al, 2013); respiratory rate less frequently measured than blood pressure and pulse (Kamio et al, 2018); and poor documentation of respiratory rate (Boerma et al, 2017). Studies examining the neglect of vital signs assessment have identified a variety of contributing factors. Although most of these studies have been small and conducted at a single site, to date there has been no published attempt to categorise these factors or show how they interrelate. This article presents a concept map highlighting the key contributing/causative factors and the relationships between them.
Concept map
Informed by contemporary and older research, the concept map highlights the main factors contributing to the neglect of vital signs assessment (Figure 1). Older research evidence was included as the neglect of vital signs assessment is an enduring clinical problem. For example, a study published more than 20 years ago on 344 patients in one UK hospital found no recording of respiratory rate in 53% of patients (Helliwell et al, 2002). Similarly, a recent integrative review of 19 studies concluded that respiratory rates are not being assessed correctly in clinical practice (Palmer et al, 2023).
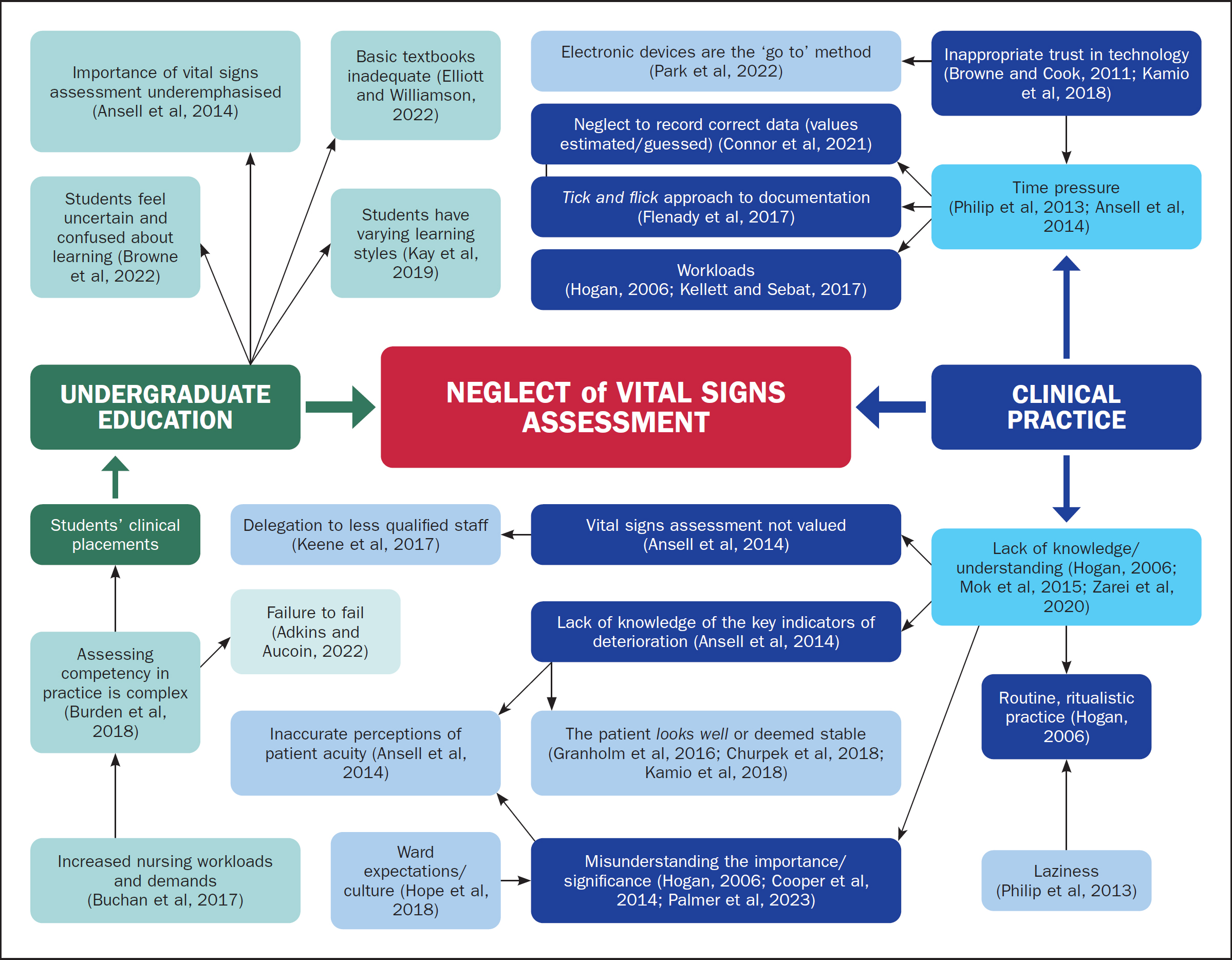
The factors contributing to the neglect of vital signs assessment are divided into two groups: undergraduate education and clinical practice. The experience of being an undergraduate student is influenced by many factors. Nursing students are under pressure to comprehend a large volume of theoretical knowledge, develop competence in clinical skills, and also pass their academic and clinical assessments. Many factors also influence the experience of being an adult learner at university. The concept map cannot present all of them but key factors are cited. Other factors influencing the experience of being a nursing student include the ability to meet challenges, intrinsic motivation, perseverance, passion and commitment to long term goals (Jeffreys, 2015; Khalaila, 2015; Duckworth, 2016; Terry and Peck, 2020; Halperin and Eldar Regev, 2021).
The assessment of vital signs in clinical practice is also influenced by many variables. The key factors are cited in the map and primarily involve a lack of understanding of the importance of vital signs assessment. It is not evident where this ignorance begins. Undergraduate nursing students might perceive the skill as simply one of many they must develop or its importance might be underemphasised (Ansell et al, 2014). If students graduate with a misunderstanding of vital signs assessment, it is likely this is reinforced by the culture and practice they encounter at the bedside (such as the factors cited in Figure 1).
Limitations
The development of this concept map was informed by contemporary and past research. Older studies were cited as the neglect of vital signs assessment is an enduring problem. Although there are common research findings between studies, some of the findings are from small, single-site studies.
Discussion
Vital signs assessment is a critical process in the safe delivery of clinical care. The concept map attempts to show the complex inter-relationships between the many variables influencing the neglect of vital signs assessment practices. The map has application to undergraduate and clinical education. Vital signs assessment is a multifaceted issue which, despite research on the topic, is an enduring problem in clinical practice. To the authors’ knowledge, this is the first publication that has attempted to highlight factors contributing to the neglect of vital signs assessment and show how they inter-relate.
The accurate assessment of vital signs is essential to the success of early warning scores and rapid response systems (Kallioinen et al, 2021). Abnormal vital signs, for instance, have been associated with increased risk for critical events (Lighthall et al, 2009). It is therefore important that nurses be educated on the importance of early identification of clinical deterioration (Kamio et al, 2018). This concept map is a tool that can help plan and scaffold educational resources.
How can the enduring neglect of vital signs assessment be explained or rationalised? Vital signs are vital, so why is their assessment not prioritised? By now one would have thought that the monitoring of vital signs should be a fundamental part of healthcare practice and performed perfectly (Wong, 2018). The concept map shows the many factors contributing to the problem. It could simply be that, despite the title, students and then registered nurses lack the knowledge to realise the critical importance of vital signs assessment. It is possible that nurses’ lack of awareness of the ‘vitalness’ of vital signs starts at undergraduate level. This lack of awareness might then be reinforced by assessment behaviours or the culture they encounter in clinical practice. Overall, many of the contributing factors relate to awareness or understanding, which are primarily education issues.
A second explanation for the neglect of vital signs assessment might be the power of group behaviour. When people operate in groups, such as a cohort of nurses employed on a ward, they do not engage in nuanced thinking and deep analysis (Greene, 2018). ‘Around others…we feel pressure to fit in, and to do so, we begin to shape our thoughts and beliefs to the group orthodoxies. We unconsciously imitate others in the group…’ (Greene, 2018). As mentioned above, new graduates or new staff may be influenced by the culture they encounter in clinical practice.
A third explanation might relate to human behaviour, which has been described as ‘predictably irrational’ (Ariely, 2008). Patient safety is underpinned by assessment, and assessment is typically included in national nursing standards (eg those from the Nursing and Midwifery Board of Australia (2016) or the UK's Nursing and Midwifery Council (2024)). Why, then, would a registered nurse choose to neglect to do an assessment that is deemed vital, particularly when assessment is a national nursing standard? The reasons for this are unclear but could also to relate to the human brain's ability to justify behaviour that defies logic, guidelines or rational explanation. It has also been suggested that under high cognitive load, the human brain resorts to taking shortcuts and making decisions based on stereotypes (Kahneman, 2011). For example, in an Australian study involving 79 emergency department nurses, informants reported using various strategies to rationalise their transgressions against standard clinical practice regarding vital signs assessment (Flenady et al, 2017). These included valuing clinical experience over organisational requirements and justifying their errant behaviour (Flenady et al, 2017).
Application and relevance
The concept map provides a global view of the neglect of vital signs assessment. It highlights the various factors contributing to this neglect and the relationships between them. These are key factors to target for improving nurses’ vital signs assessment practices. Most of the factors in the map reflect a poor understanding of the importance of vital signs assessment. The map can therefore be used as a framework for designing educational interventions for undergraduate nursing curricula and graduate nurses. The map is also a framework for future research. For example, research could trial innovative methods for teaching vital signs assessment to nursing students. Action research could also empower nurses to change vital signs assessment culture at the ward level.
Conclusion
The neglect of vital signs assessment is an enduring problem in clinical practice. Many factors in the undergraduate and clinical areas contribute to this, as presented in the concept map. The factors mostly seem to relate a lack of awareness or understanding of the importance of vital signs.